The PDF editor was created with the aim of allowing it to be as effortless and intuitive as possible. All of these actions will make creating the capf 160 pdf easy and quick.
Step 1: The following webpage has an orange button that says "Get Form Now". Merely click it.
Step 2: The form editing page is now open. You can include text or enhance current data.
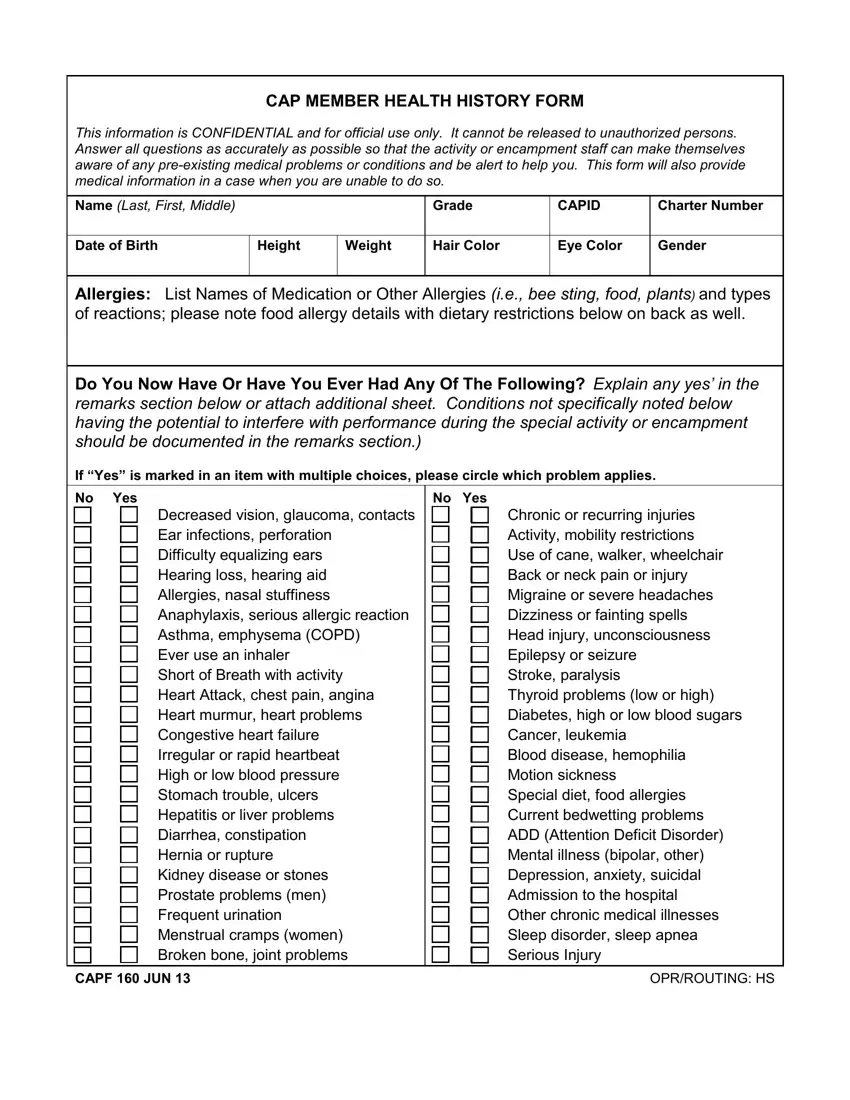
Complete the capf 160 pdf PDF and enter the content for every area:
Write down the requested details in Decreased vision glaucoma contacts, Irregular or rapid heartbeat High, Chronic or recurring injuries, CAPF JUN, and OPRROUTING HS box.
The program will require you to insert some necessary info to instantly fill in the part Dietary Restrictions or, Past Surgical History List all, Date Tetanus Booster, Hepatitis Vaccine, No Td or Tdap, Date, Date, Pneumonia Vaccine No, Date, Varicella Immuni zationchickenpox, Influenza Vaccine, Date, Date, Medication Information Include, and Name of MedicationInhaler.
You will need to identify the rights and responsibilities of every party in part Tobacco Use packs per day years, Occupation student or other, Religious Preference, Social History, Remarks Attach additional sheet if, CONSENT FOR MINOR CADET, I give permission for full, My signature below evidences my, and In case of emergency I understand.
Step 3: Press the "Done" button. Now, you may transfer the PDF file - upload it to your device or send it by means of email.
Step 4: It's possible to make duplicates of the file toremain away from any upcoming problems. You need not worry, we cannot distribute or check your information.
