The Care Expense Statement form is a critical document designed to provide a comprehensive overview of the care-related expenses for veterans or other individuals requiring varying levels of care. This form, meticulously divided into sections, collects detailed information starting from general personal and facility details in Section 1, extending to specific care types—ranging from in-home care to specialized facilities such as nursing homes, foster homes, adult day cares, rest homes, group homes, and assisted living environments—in the subsequent sections. It requires the facility administrator or care provider to fill in pertinent details such as the care recipient's name, the nature and duration of care, the total monthly charges, and any financial assistance or insurance coverage the patient may be receiving, including Medicaid, Medicare, or private insurance. Additionally, the form delves into the specifics of the care provided, asking whether the facility offers medical or nursing services and if such services are facilitated by a licensed health professional. It goes further to break down the cost into base rates and medical or nursing service charges, aiming at complete transparency regarding the patient’s care expenditure. The form concludes with a section for signatures, ensuring all information provided is verified and accurate to the best knowledge of both the facility administrator or care provider and the veteran or beneficiary. This level of detail not only helps in maintaining records but also assists in the application for financial aid and reimbursement processes, providing a structured format for the veterans or their families to understand and manage their care expenses effectively.
| Question | Answer |
|---|---|
| Form Name | Care Expense Statement Form |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | va child care letter fillable, care expense statement, irs form 8049, expense statement home |
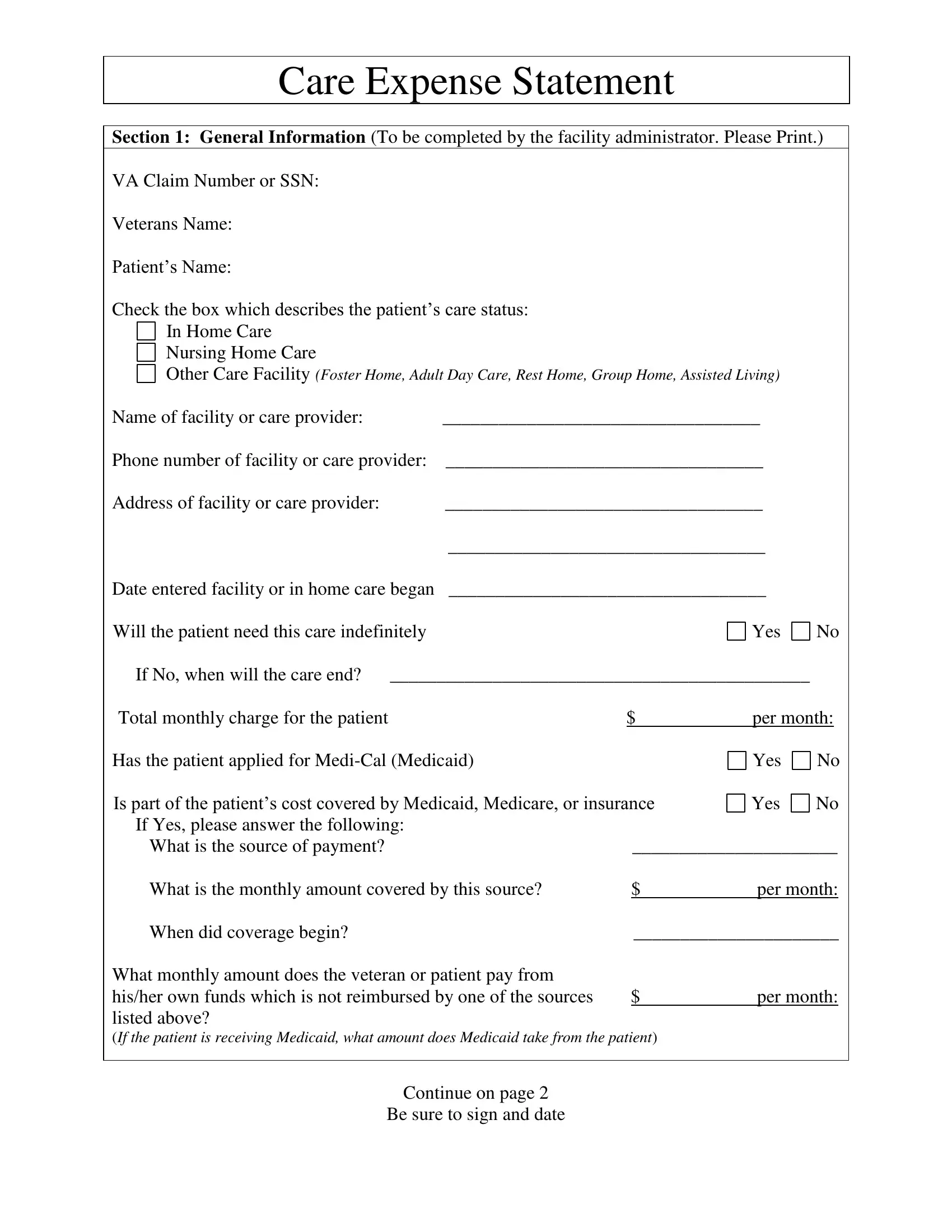
Care Expense Statement
Section 1: General Information (To be completed by the facility administrator. Please Print.)
VA Claim Number or SSN:
Veterans Name:
Patient’s Name:
Check the box which describes the patient’s care status:
In Home Care
Nursing Home Care
Other Care Facility (Foster Home, Adult Day Care, Rest Home, Group Home, Assisted Living)
Name of facility or care provider: |
|
__________________________________ |
|
|
|||
Phone number of facility or care provider: __________________________________ |
|
|
|||||
Address of facility or care provider: |
|
__________________________________ |
|
|
|||
|
|
__________________________________ |
|
|
|||
Date entered facility or in home care began |
__________________________________ |
|
|
||||
Will the patient need this care indefinitely |
|
|
|
Yes |
No |
||
If No, when will the care end? |
_____________________________________________ |
|
|
||||
Total monthly charge for the patient |
|
|
$ |
per month: |
|
||
Has the patient applied for |
|
|
Yes |
No |
|||
Is part of the patient’s cost covered by Medicaid, Medicare, or insurance |
Yes |
No |
|||||
If Yes, please answer the following: |
|
|
|
|
|
|
|
What is the source of payment? |
|
|
______________________ |
||||
What is the monthly amount covered by this source? |
|
$ |
per month: |
||||
When did coverage begin? |
|
|
______________________ |
||||
What monthly amount does the veteran or patient pay from |
|
|
|
|
|
||
his/her own funds which is not reimbursed by one of the sources |
$ |
per month: |
|||||
listed above? |
|
|
|
|
|
|
|
(If the patient is receiving Medicaid, what amount does Medicaid take from the patient)
Continue on page 2
Be sure to sign and date
Section 2:
(To be completed by the care provider only if patient is being provided
Do You provide any medical or nursing services for the patient?
Yes
No
(i.e. administering medication, physical or mental therapy, assisting with personal hygiene, dressing bathing; etc.)
Describe the services you provide:_________________________________________________
Are you a licensed health professional? (RN, LVN or LPN) |
Yes |
No |
If Yes, provide your license number: ________________________________________
Section 3: Nursing Home Information
(To be completed by the facility administrator only if the patient is in a nursing home.)
Is your facility licensed by the State?
Is your facility Medicaid
Yes
Yes
No
No
Is the patient in your nursing home because of a physical or mental disability? |
Yes |
No |
Do you provide either skilled or intermediate level nursing care to the patient? |
Yes |
No |
What was the admitting diagnosis? _______________________________________________
Section 4: Other Care Facility Information
( To be completed by the facility administrator only if the patient is in a foster home, adult day care, rest home, group home or assisted living)
Indicate type of facility |
Assisted Living |
Rest Home |
|
Adult Day Care |
Group Home |
||
|
Do you provide any medical or nursing services for the patient?
Foster Home
Other _____________
Yes No
(i.e. administering medication, physical or mental therapy, assisting with personal hygiene, dressing bathing; etc.)
Describe the services you provide: ________________________________________________
If the patient receives medical or nursing services, are the services |
|
|
Yes |
No |
|
provided or supervised by a licensed health professional (RN, LVN, LPN) |
|
|
|||
We must have the monthly charge broken down into the following categories: |
|
|
|||
1. |
Base Rate (includes room, meals, laundry, housekeeping): $ |
per month: |
|||
|
|
|
|
|
|
2. |
Medical and Nursing Services: |
$ |
per month: |
||
Section 5: Signatures (To be completed by the facility administrator/care provider and veteran/widow)
I certify that the above statements are true and correct to the best of my knowledge and belief.
___________________________________________________ |
__________________________________ |
Signature of facility administrator or care provider |
Date |
I certify that the above statements are true and correct to the best of my knowledge and belief. I am paying $_________ per month for my care from my own funds.
___________________________________________________ |
__________________________________ |
Signature of Veteran or Beneficiary |
Date |