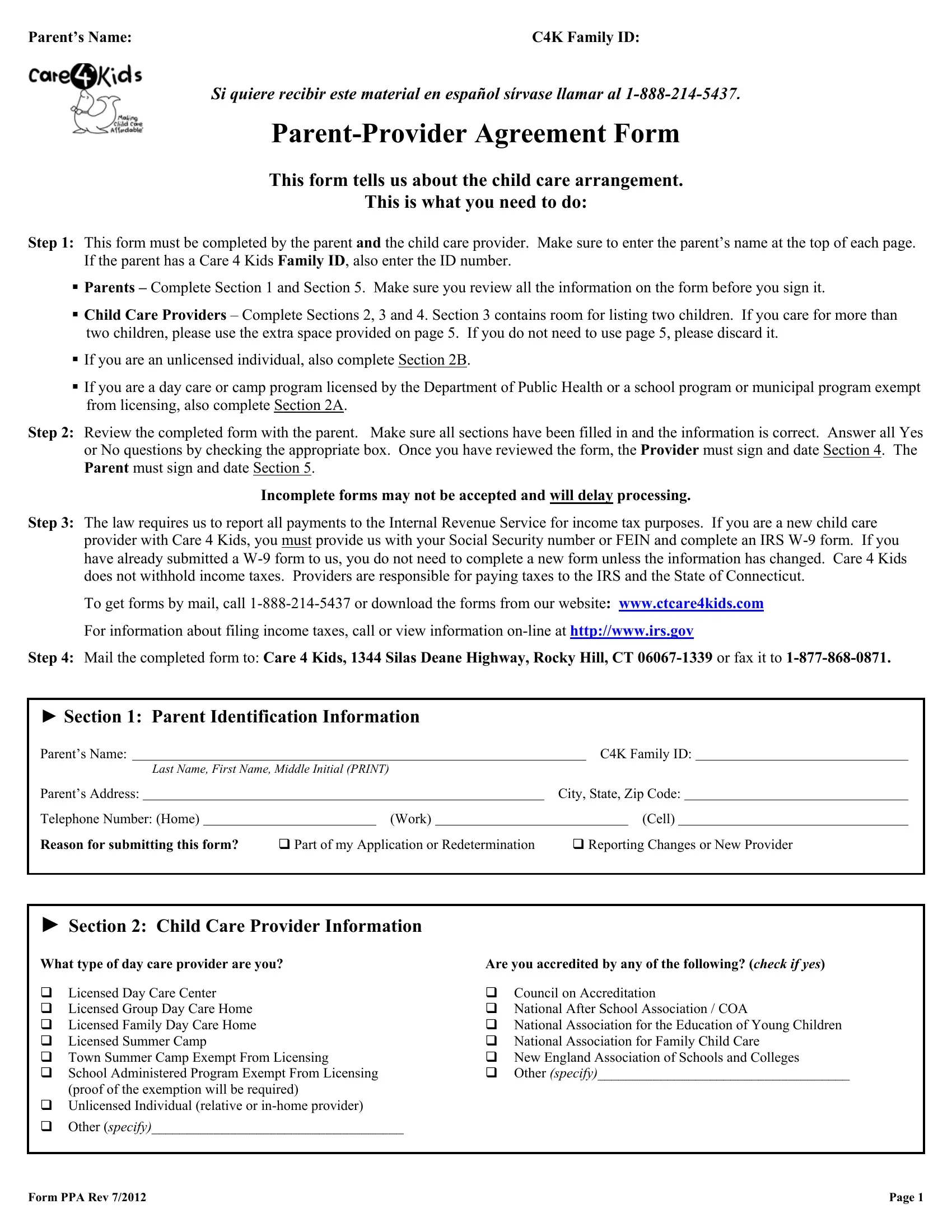
In navigating the complexities of child care assistance, the Care4Kids Parent-Provider Agreement (PPA) form serves as a fundamental tool for families and providers within Connecticut. This comprehensive document outlines the procedural steps and requirements for both parents and child care providers to establish a formal arrangement under the Care 4 Kids program. Initially, the form mandates collaborative completion by the parent—who provides crucial identification details and reasons for submission—and the child care provider, who offers information regarding the care setting, accreditation, and services provided. The PPA form is designed to facilitate clear communication and agreements concerning child care arrangements, payment responsibilities, and schedules, ensuring that the care provided aligns with state regulations and standards. Moreover, it encompasses vital sections on child care provider information, including certifications and background checks, as a measure to guarantee the safety and well-being of the children under their care. The procedure laid out by the form also includes steps for legal compliance with tax reporting requirements to the Internal Revenue Service, highlighting the formal and regulated nature of these care arrangements. Through an exhaustive process of review, signature by both parties, and submission guidelines, the form plays an indispensable role in the structured and efficient administration of child care services, thereby supporting both the developmental needs of children and the operational demands of providers within the Care 4 Kids program.
| Question | Answer |
|---|---|
| Form Name | Care4Kids Form Ppa |
| Form Length | 5 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 1 min 15 sec |
| Other names | C4KfinalPPA connecticut kids parents form |
Parent’s Name: |
C4K Family ID: |
Si quiere recibir este material en español sírvase llamar al
This form tells us about the child care arrangement.
This is what you need to do:
Step 1: This form must be completed by the parent and the child care provider. Make sure to enter the parent’s name at the top of each page. If the parent has a Care 4 Kids Family ID, also enter the ID number.
Parents – Complete Section 1 and Section 5. Make sure you review all the information on the form before you sign it.
Child Care Providers – Complete Sections 2, 3 and 4. Section 3 contains room for listing two children. If you care for more than two children, please use the extra space provided on page 5. If you do not need to use page 5, please discard it.
If you are an unlicensed individual, also complete Section 2B.
If you are a day care or camp program licensed by the Department of Public Health or a school program or municipal program exempt from licensing, also complete Section 2A.
Step 2: Review the completed form with the parent. Make sure all sections have been filled in and the information is correct. Answer all Yes or No questions by checking the appropriate box. Once you have reviewed the form, the Provider must sign and date Section 4. The Parent must sign and date Section 5.
Incomplete forms may not be accepted and will delay processing.
Step 3: The law requires us to report all payments to the Internal Revenue Service for income tax purposes. If you are a new child care provider with Care 4 Kids, you must provide us with your Social Security number or FEIN and complete an IRS
To get forms by mail, call
For information about filing income taxes, call or view information
Step 4: Mail the completed form to: Care 4 Kids, 1344 Silas Deane Highway, Rocky Hill, CT
► Section 1: Parent Identification Information
Parent’s Name: |
|
|
|
|
C4K Family ID: |
|||||||
|
|
Last Name, First Name, Middle Initial (PRINT) |
|
|
|
|
|
|
||||
Parent’s Address: |
|
|
|
|
City, State, Zip Code: |
|
||||||
Telephone Number: (Home) |
|
|
(Work) |
|
|
|
(Cell) |
|
||||
Reason for submitting this form? |
Part of my Application or Redetermination |
Reporting Changes or New Provider |
||||||||||
► Section 2: Child Care Provider Information
What type of day care provider are you? |
Are you accredited by any of the following? (check if yes) |
||
Licensed Day Care Center |
|
Council on Accreditation |
|
Licensed Group Day Care Home |
National After School Association / COA |
||
Licensed Family Day Care Home |
National Association for the Education of Young Children |
||
|
Licensed Summer Camp |
National Association for Family Child Care |
|
Town Summer Camp Exempt From Licensing |
New England Association of Schools and Colleges |
||
School Administered Program Exempt From Licensing |
|
Other (specify)____________________________________ |
|
|
(proof of the exemption will be required) |
|
|
Unlicensed Individual (relative or |
|
|
|
|
Other (specify)____________________________________ |
|
|
Form PPA Rev 7/2012 |
Page 1 |
Parent’s Name: |
C4K Family ID: |
►Section 2A: Licensed Child Care Providers, Schools and Camp Programs
Provider Name: _________________________________________________Social Security or Federal Tax ID Number:
Address where care is provided: ______________________________________ City, State, Zip Code:
Your Telephone Number: |
|
Date of Birth (Family Home Providers Only): |
|
||
C4K Provider ID: |
|
|
DPH License Number: |
|
|
Please list the address you would like notices or checks to be mailed if different from the address where care is provided:
Notices/Invoices: |
|
City, State, Zip Code: |
|
Checks/Payments: |
|
City, State, Zip Code: |
|
►Section 2B: Unlicensed Relatives and
You must be a close relative to provide child care in your home. Close relative means the child is your grandchild, great grandchild, sibling, niece, nephew, great niece, great nephew, first cousin or second cousin. If you are not a close relative, you must have a license from the Department of Public Health to provide child care in your home.
Provider Name: |
|
Social Security or Federal Tax ID Number: |
|
|||||
Home Address: |
|
City, State, Zip Code: |
|
|||||
Your Telephone Number: |
|
C4K Provider ID: |
|
|||||
What is your Date of Birth? |
|
Sex: |
Male Female |
|||||
What is the maximum number of children in your care at the same time on any day, including your own children?
How many of the children are under the age of 2, including your own children?
Are you |
Yes No |
Name, Address & Telephone Number of Your Employer:
Use this table to show us the hours and days you normally work at your other job (circle AM or PM).
|
SUNDAY |
MONDAY |
TUESDAY |
WEDNESDAY |
THURSDAY |
FRIDAY |
SATURDAY |
FROM |
AM PM |
AM PM |
AM PM |
AM PM |
AM PM |
AM PM |
AM PM |
|
|
|
|
|
|
|
|
TO |
AM PM |
AM PM |
AM PM |
AM PM |
AM PM |
AM PM |
AM PM |
|
|
|
|
|
|
|
|
Where do you provide care for the children listed in this agreement form? Child’s Home Provider’s Home Other
Is there a working telephone at this address? Yes No Telephone number and area code:
Is this a cell phone? Yes No If yes, name of person who owns the cell phone:
If you use a cell phone, the cell phone must be in your name or part of a family share plan with multiple phone lines.
Is there a working smoke detector? Yes No |
Do you have immediate access to a fire extinguisher? Yes No |
Are you under investigation for child abuse or child neglect or do you have a record of child abuse or neglect in Connecticut or in any other state?
Yes No
Were you ever arrested or do you have an arrest warrant or criminal charge pending against you? Yes No What crime were you charged with, when and where?
Have you ever been convicted of any of the crimes listed below? Yes |
No |
Abandonment, injury or risk of injury to a minor |
Crimes involving a weapon, explosives or a firearm |
Cruelty to persons or animals, stalking, obscenity, public |
Sex crimes, including sexual assault, rape, prostitution, child |
indecency, reckless endangerment, arson, robbery, burglary, |
pornography and other related sex crimes |
home invasion |
|
Use of force against another person, including murder, assault, |
Sale, manufacture or possession of narcotics or other illegal drugs |
manslaughter, kidnapping, unlawful restraint |
or controlled substances |
Note: All Unlicensed Providers are subject to child abuse or neglect and criminal background checks.
Form PPA Rev 7/2012 |
Page 2 |
Parent’s Name: |
C4K Family ID: |
►Section 3: Children In Care (Complete for each child needing Care 4 Kids assistance.)
CHILD 1 - Full Name: |
|
|
|
|
|
Date of Birth: |
|
|
|
||
Date care started: |
|
|
|
How much do you charge the parent per week? $ |
|
|
|||||
|
|
|
|
|
|
|
|
||||
Do you provide care for this child before or after school? (Check boxes) |
Before School |
After School |
|
|
|||||||
Licensed Providers: Do you receive funding from any other source for this child? Check all that apply: |
|
|
|||||||||
School Readiness |
State Head Start |
Federal Head Start |
DSS CDC |
DSS BAS |
|||||||
Relative and |
Are you related to this child? |
Yes No |
If related, specify your relationship below: |
||||||||
Grandparent/Great Grandparent |
Aunt/Uncle |
Sibling Niece/Nephew First Cousin/Second Cousin Other: |
|
||||||||
CHILD’S CARE SCHEDULE: Fill in the time the child is in your care (Circle AM or PM).
|
SUNDAY |
MONDAY |
TUESDAY |
WEDNESDAY |
THURSDAY |
FRIDAY |
SATURDAY |
FROM |
AM PM |
AM PM |
AM PM |
AM PM |
AM PM |
AM PM |
AM PM |
TO
AM PM
AM PM
AM PM
AM PM
AM PM
AM PM
AM PM
FROM
AM PM
AM PM
AM PM
AM PM
AM PM
AM PM
AM PM
TO
AM PM
AM PM
AM PM
AM PM
AM PM
AM PM
AM PM
Is the schedule the same each week? |
Yes No If no, explain how the schedule varies: |
|
|
|
|
►Section 3: Children In Care (Complete for each child needing Care 4 Kids assistance.)
CHILD 2 - Full Name: |
|
|
|
|
|
Date of Birth: |
|
|
|
||
Date care started: |
|
|
|
How much do you charge the parent per week? $ |
|
|
|||||
|
|
|
|
|
|
|
|
||||
Do you provide care for this child before or after school? (Check boxes) |
Before School |
After School |
|
|
|||||||
Licensed Providers: Do you receive funding from any other source for this child? Check all that apply: |
|
|
|||||||||
School Readiness |
State Head Start |
Federal Head Start |
DSS CDC |
DSS BAS |
|||||||
Relative and |
Are you related to this child? |
Yes No |
If related, specify your relationship below: |
||||||||
Grandparent/Great Grandparent |
Aunt/Uncle |
Sibling Niece/Nephew First Cousin/Second Cousin Other: |
|
||||||||
CHILD’S CARE SCHEDULE: Fill in the time the child is in your care (Circle AM or PM).
|
SUNDAY |
MONDAY |
TUESDAY |
WEDNESDAY |
THURSDAY |
FRIDAY |
SATURDAY |
FROM |
AM PM |
AM PM |
AM PM |
AM PM |
AM PM |
AM PM |
AM PM |
TO
AM PM
AM PM
AM PM
AM PM
AM PM
AM PM
AM PM
FROM
AM PM
AM PM
AM PM
AM PM
AM PM
AM PM
AM PM
TO
AM PM
AM PM
AM PM
AM PM
AM PM
AM PM
AM PM
Is the schedule the same each week? |
Yes No If no, explain how the schedule varies: |
|
|
|
|
Form PPA Rev 7/2012 |
Page 3 |
Parent’s Name: |
C4K Family ID: |
►Section 4: Provider Certification: (To be Completed by the Child Care Provider.)
To the best of my knowledge, I certify that:
1)I am the individual or program that is providing care to the children listed on this form. I am at least 18 years of age and capable of providing safe and competent child care services. I do not have a disability, impairment or health problem that would prevent me from caring for the children.
2)Care will be given at the location specified on the form. I am responsible for reporting changes in the hours of care, the amount I charge for services, if the child stops attending care and changes in the location where care is given. I must also inform Care 4 Kids of any changes in my criminal or child abuse/neglect history. Changes must be reported by telephone or in writing by the date the first billing invoice is submitted to Care 4 Kids following the change.
3)For each child in my care, I have the name of the child’s primary care physician and health insurance provider and proof that each child is up to date with his or her immunizations and health screening exams.
4)I understand and agree that the Department of Social Services and Care 4 Kids may verify information listed on this form independently without prior authorization, including criminal and child abuse/neglect background checks.
5)I understand that this agreement is between the parent and the provider. It is not a contract with Care 4 Kids or the State of Connecticut. Neither Care 4 Kids nor the State of Connecticut employs me.
6)Care 4 Kids may not cover my total charges. The parent is responsible for any costs that are not paid by Care 4 Kids.
7)I may be required to repay benefits that were paid to me in error. I may also be subject to criminal or civil charges if I knowingly omit, misrepresent or provide false information to Care 4 Kids or if I do not timely report changes affecting payments or my eligibility for this program. I may be liable for all penalties associated with crimes, including, but not limited to, larceny by defrauding a public community, conspiracy to commit larceny by defrauding a public community, vendor fraud, forgery, false statement and other relevant crimes pursuant to Title 53a of the Connecticut General Statutes.
8)I must submit a completed invoice to receive payment. Invoices will be sent to me when payment is approved and monthly thereafter. I will have 120 days to return the completed invoice in order to be paid.
9)To be eligible for payments, I will cooperate with the Department of Social Services and its designees in program audits and fraud prevention activities, including any site visits that may be conducted to my home, child care site or place of employment.
10)I have read and understand the information contained in this form and certify that all of the information I have provided is true and correct to the best of my knowledge.
Provider Name (please print):
Provider Signature: |
|
Date: |
Witness’ Signature (If the provider signs with an “X”):
►Section 5: Parent Certification: (To be Completed by the Parent.)
I certify that:
1)I have selected the provider identified above to care for my children while I work or attend an approved activity.
2)I will report any changes in child care arrangements, income, activity, people living in my home, or my residential address to Care 4 Kids within 10 days of a change.
3)I am responsible to pay the provider any costs not covered by Care 4 Kids.
4)I understand and agree that Care 4 Kids may contact the provider listed above and the provider may contact Care 4 Kids concerning my eligibility and payment amounts.
5)I may be required to repay benefits that were paid in error on my behalf. I may also be subject to criminal or civil charges if I knowingly omit, misrepresent or provide false information to Care 4 Kids or if I do not timely report changes affecting payments or my eligibility for this program. I may be liable for all penalties associated with crimes including but not limited to larceny by defrauding a public community, conspiracy to commit larceny by defrauding a public community, vendor fraud, forgery, false statement and other relevant crimes pursuant to Title 53a of the Connecticut General Statutes.
Parent Name (please print):
Parent Signature: |
|
Date: |
Form PPA Rev 7/2012 |
Page 4 |
Parent’s Name: |
C4K Family ID: |
Use This Page If The Family Has More Than Two Children In Your Care
►Section 3: Supplement For Additional Children In Care
CHILD 3 - Full Name: |
|
|
|
|
|
Date of Birth: |
|
|
|
||
Date care started: |
|
|
|
How much do you charge the parent per week? $ |
|
|
|||||
|
|
|
|
|
|
|
|
||||
Do you provide care for this child before or after school? (Check boxes) |
Before School |
After School |
|
|
|||||||
Licensed Providers: Do you receive funding from any other source for this child? Check all that apply: |
|
|
|||||||||
School Readiness |
State Head Start |
Federal Head Start |
DSS CDC |
DSS BAS |
|||||||
Relative and |
Are you related to this child? |
Yes No |
If related, specify your relationship below: |
||||||||
Grandparent/Great Grandparent |
Aunt/Uncle |
Sibling Niece/Nephew First Cousin/Second Cousin Other: |
|
||||||||
CHILD’S CARE SCHEDULE: Fill in the time the child is in your care (Circle AM or PM).
|
SUNDAY |
MONDAY |
TUESDAY |
WEDNESDAY |
THURSDAY |
FRIDAY |
SATURDAY |
FROM |
AM PM |
AM PM |
AM PM |
AM PM |
AM PM |
AM PM |
AM PM |
TO
AM PM
AM PM
AM PM
AM PM
AM PM
AM PM
AM PM
FROM
AM PM
AM PM
AM PM
AM PM
AM PM
AM PM
AM PM
TO
AM PM
AM PM
AM PM
AM PM
AM PM
AM PM
AM PM
Is the schedule the same each week? |
Yes No If no, explain how the schedule varies: |
|
|
|
|
►Section 3: Supplement For Additional Children In Care
CHILD 4 - Full Name: |
|
|
|
|
|
Date of Birth: |
|
|
|
||
Date care started: |
|
|
|
How much do you charge the parent per week? $ |
|
|
|||||
|
|
|
|
|
|
|
|
||||
Do you provide care for this child before or after school? (Check boxes) |
Before School |
After School |
|
|
|||||||
Licensed Providers: Do you receive funding from any other source for this child? Check all that apply: |
|
|
|||||||||
School Readiness |
State Head Start |
Federal Head Start |
DSS CDC |
DSS BAS |
|||||||
Relative and |
Are you related to this child? |
Yes No |
If related, specify your relationship below: |
||||||||
Grandparent/Great Grandparent |
Aunt/Uncle |
Sibling Niece/Nephew First Cousin/Second Cousin Other: |
|
||||||||
CHILD’S CARE SCHEDULE: Fill in the time the child is in your care (Circle AM or PM).
|
SUNDAY |
MONDAY |
TUESDAY |
WEDNESDAY |
THURSDAY |
FRIDAY |
SATURDAY |
FROM |
AM PM |
AM PM |
AM PM |
AM PM |
AM PM |
AM PM |
AM PM |
TO
AM PM
AM PM
AM PM
AM PM
AM PM
AM PM
AM PM
FROM
AM PM
AM PM
AM PM
AM PM
AM PM
AM PM
AM PM
TO
AM PM
AM PM
AM PM
AM PM
AM PM
AM PM
AM PM
Is the schedule the same each week? |
Yes No If no, explain how the schedule varies: |
|
|
|
|
Form PPA Rev 7/2012 |
Page 5 |