We have used the efforts of our best programmers to build the PDF editor you intend to apply. The software allows you to fill in the case document forms document effortlessly and don’t waste precious time. All you should undertake is follow the following easy tips.
Step 1: The following website page contains an orange button stating "Get Form Now". Select it.
Step 2: After you have entered the case document forms editing page you'll be able to discover all of the options you may conduct concerning your file from the upper menu.
For every single part, add the information demanded by the program.
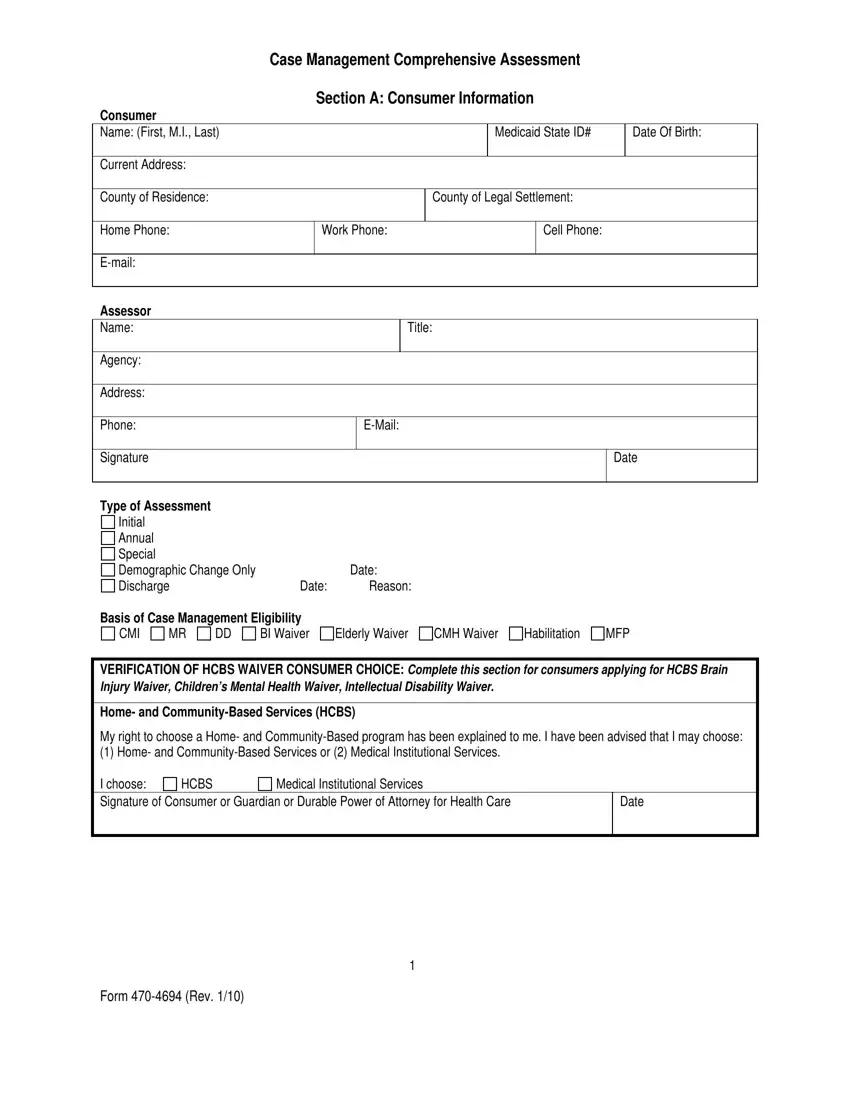
Note the appropriate information in Basis of Case Management, CM, I BI Waiver, Elderly Waiver CM, H Waiver, VERIFICATION OF H, CBS WAIVER, Home- and Community, Based Services, My right to choose a Home- and, Medical Institutional Services, H, CBS, Date, and Form 470, 4694 (Rev area.
Note down the significant particulars when you're within the Name, Title (if applicable), Relationship to Consumer, Additional records reviewed:, Female, Male, Comments: Monthly Income: (Please, Source, SSI S, SDI Employment Other, Yes, and Amount section.
The SSI S, SDI Employment Other, Comments: Court Involvement:, Involuntary Commitment Probation, and Comments: box will be the place to indicate the rights and obligations of each side.
Finish by reading the following fields and preparing them correspondingly: Consumer Name: Legal decision, None, Guardian, Attorney, in, fact Other (Specify):, Name: (First, Work Phone:, Cell Phone:, Guardian, Attorney, in, fact Other (Specify):, Cell Phone:, Yes, (complete below), and Work Phone:.
Step 3: When you are done, choose the "Done" button to upload your PDF form.
Step 4: Generate copies of your document. This is going to prevent possible challenges. We cannot see or publish your details, thus you can relax knowing it is protected.
