Within the complexities of correctional facilities and parole environments, ensuring equal access and opportunities for those with disabilities embodies a fundamental principle of justice and equality. This principle is upheld through instruments like the CDCR 1824 form, a document that plays a pivotal role in the lives of inmates and parolees with disabilities within the State of California's Department of Corrections and Rehabilitation. The form serves as a formal request for reasonable modifications or accommodations, ensuring compliance with the Americans With Disabilities Act (ADA). It aims to prevent discrimination by enabling qualified individuals with disabilities to participate fully in the services, activities, or programs offered by the respective institution or facility. The process detailed in the form is straightforward yet impactful: it requires the submission of a completed request to an Appeals Coordinator's Office, followed by a structured review process that endeavors to return decisions within a concise timeframe. Furthermore, if disagreements arise concerning the resolution, the form outlines a clear hierarchy of appeals to ensure that the rights of inmates and parolees are persistently respected and advocated for. By detailing specific accommodations or modifications needed, including any requests for auxiliary aids or structural adjustments, the CDCR 1824 form embodies a crucial mechanism for justice, striving to adapt the correctional environment to meet the varied and rightful needs of individuals with disabilities.
| Question | Answer |
|---|---|
| Form Name | Cdcr 1824 Form |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | specify, cdc, cdcr 1824 form, cdcr |
STATE OF CALIFORNIA |
DEPARTMENT OF CORRECTIONS AND REHABILITATION |
REASONABLE MODIFICATION OR INSTITUTION/PAROLE REGION:
ACCOMMODATION REQUEST
CDCR 1824 (Rev. 10/06)
LOG NUMBER:
CATEGORY:
18. ADA
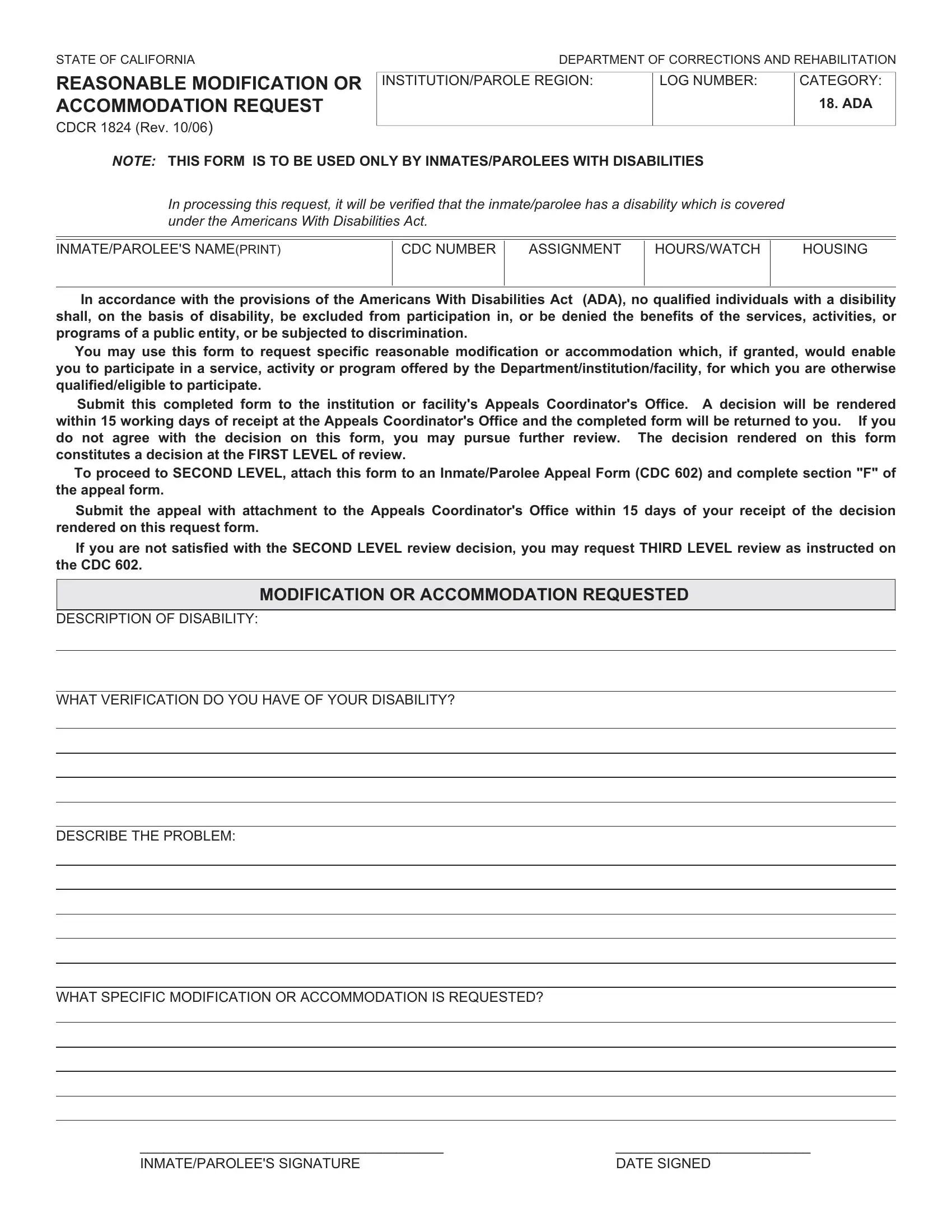
NOTE: THIS FORM IS TO BE USED ONLY BY INMATES/PAROLEES WITH DISABILITIES
In processing this request, it will be verified that the inmate/parolee has a disability which is covered under the Americans With Disabilities Act.
INMATE/PAROLEE'S NAME(PRINT)
CDC NUMBER
ASSIGNMENT
HOURS/WATCH
HOUSING
In accordance with the provisions of the Americans With Disabilities Act (ADA), no qualified individuals with a disibility shall, on the basis of disability, be excluded from participation in, or be denied the benefits of the services, activities, or programs of a public entity, or be subjected to discrimination.
You may use this form to request specific reasonable modification or accommodation which, if granted, would enable you to participate in a service, activity or program offered by the Department/institution/facility, for which you are otherwise qualified/eligible to participate.
Submit this completed form to the institution or facility's Appeals Coordinator's Office. A decision will be rendered within 15 working days of receipt at the Appeals Coordinator's Office and the completed form will be returned to you. If you do not agree with the decision on this form, you may pursue further review. The decision rendered on this form constitutes a decision at the FIRST LEVEL of review.
To proceed to SECOND LEVEL, attach this form to an Inmate/Parolee Appeal Form (CDC 602) and complete section "F" of the appeal form.
Submit the appeal with attachment to the Appeals Coordinator's Office within 15 days of your receipt of the decision rendered on this request form.
If you are not satisfied with the SECOND LEVEL review decision, you may request THIRD LEVEL review as instructed on the CDC 602.
MODIFICATION OR ACCOMMODATION REQUESTED
DESCRIPTION OF DISABILITY:
WHAT VERIFICATION DO YOU HAVE OF YOUR DISABILITY?
DESCRIBE THE PROBLEM:
WHAT SPECIFIC MODIFICATION OR ACCOMMODATION IS REQUESTED?
_______________________________________ |
_________________________ |
INMATE/PAROLEE'S SIGNATURE |
DATE SIGNED |
REASONABLE MODIFICATION OR ACCOMMODATION REQUEST |
Page 2 of 2 |
|
||
CDCR 1824 (Rev. 10/06) |
|
|
|
|
|
|
|
|
|
|
REVIEWER'S ACTION |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
DATE ASSIGNED TO REVIEWER: |
|
|
TYPE OF ADA ISSUE |
|
DATE DUE: |
|
|
|
|
|
|
|
PROGRAM, SERVICE, OR ACTIVITY ACCESS (Not requiring structural modification)
Auxiliary Aid or Device Requested
Other__________________________________________________________
PHYSICAL ACCESS (requiring structural modification)
DISCUSSION OF FINDINGS:
________________________________________ |
________________________________________ |
DATE INMATE/PAROLEE WAS INTERVIEWED |
PERSON WHO CONDUCTED INTERVIEW |
DISPOSITION |
|
|
|
|
GRANTED |
DENIED |
PARTIALLY GRANTED |
BASIS OF DECISION: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
NOTE: If disposition is based upon information provided by other staff or other resources, specify the resource and the information provided. If the request is granted, specify the process by which the modification or accommodation will be provided, with time frames if appropriate.
DISPOSITION RENDERED BY (NAME)
TITLE
INSTITUTION/FACILITY
APPROVAL
ASSOCIATE WARDEN'S SIGNATURE
DATE SIGNED
DATE RETURNED TO INMATE/PAROLEE