
Use our PDFinity® online editor to complete the authorization form quickly. The editor lets you fill in every field, add text, attach images, and sign the document electronically. Follow the steps below to complete your authorization for the release of protected health information.
Step 1: Click the "Get Form" button above to open the form in the PDF editor.
Step 2: Complete each section in the editor. Fill out patient identification, the authorizing organization, the recipient of the information, and the scope of the release.
Fill out every field accurately. Errors in patient identification, the authorization scope, or the expiration date may delay or invalidate the transfer of health information.
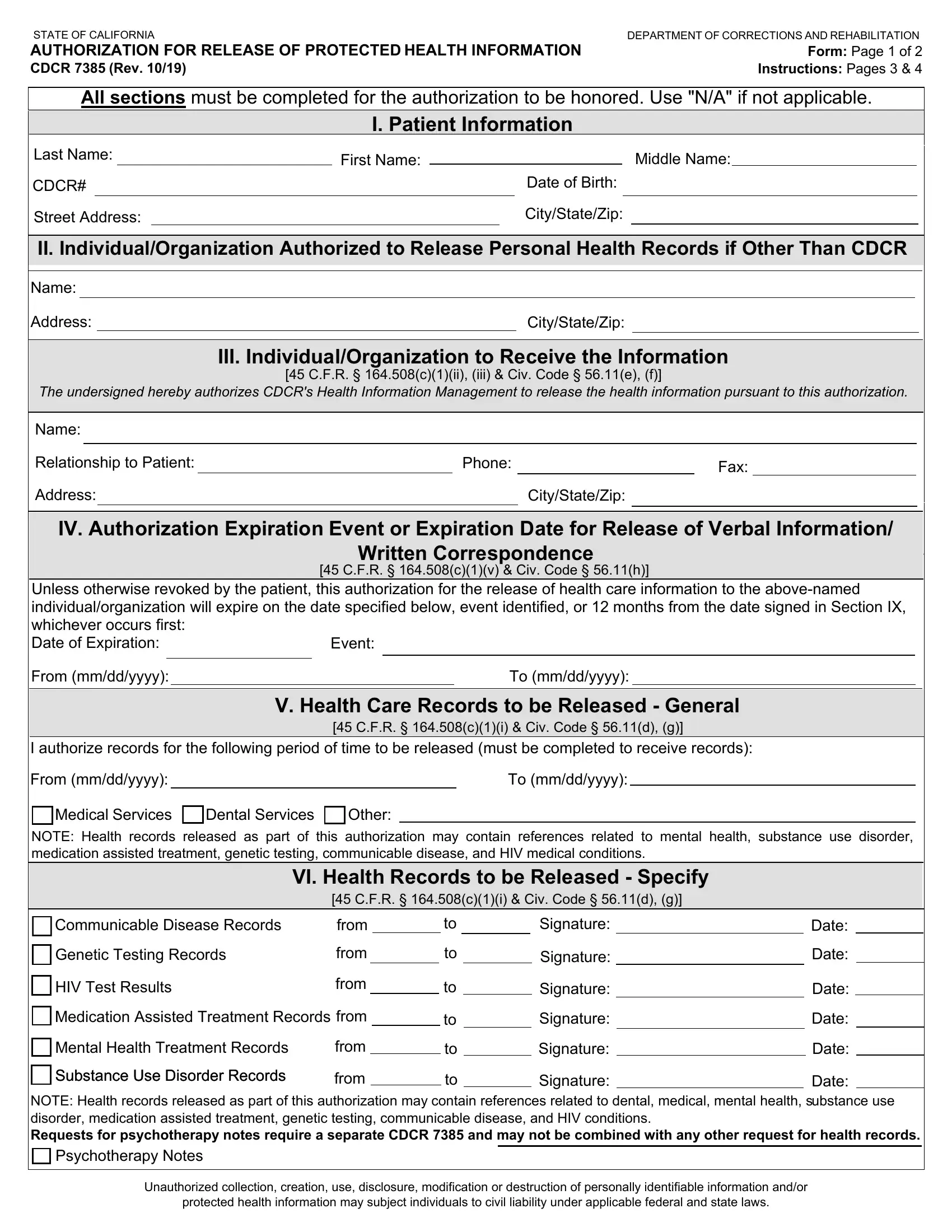
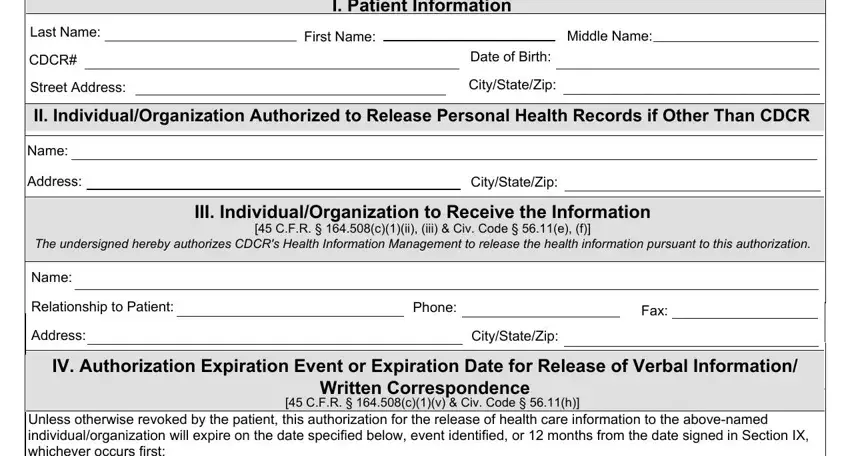
1. Begin with the top portion of the form. Enter patient identification details, the name of the correctional facility, and the organization that is authorized to disclose the protected health information:
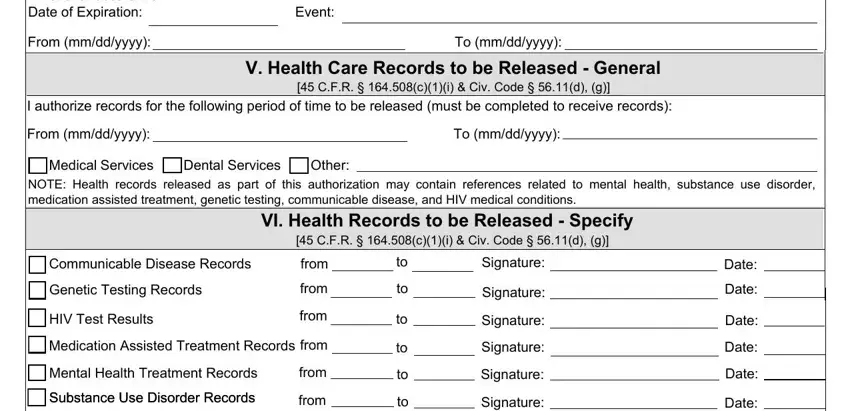
2. Complete the time period and health information sections. Specify the date range for the authorization and check the categories of health care information to be released, such as medical services, dental services, or mental health treatment data:
Pay careful attention when entering the date range and information categories. These are the most common fields where patients make errors on the authorization form.
3. Indicate whether psychotherapy notes are included. Note that psychotherapy notes require a separate patient authorization under California and federal law:

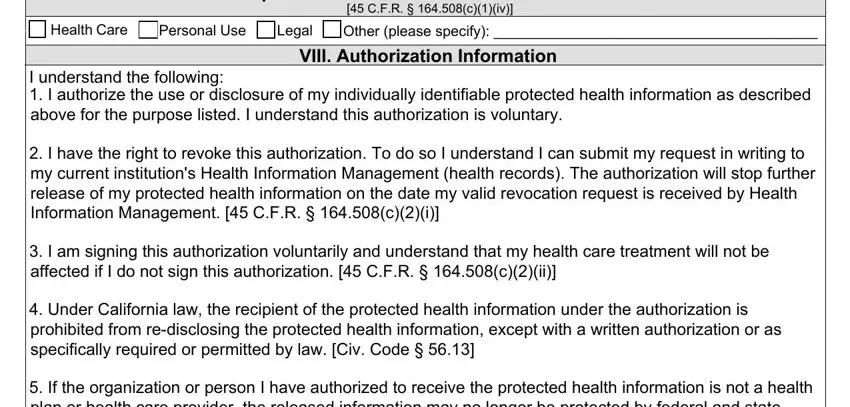
4. In Section VII, state the purpose for the release of health information. Purposes include personal use, legal proceedings, or continuation of health care. Then review Section VIII, the authorization statement, and confirm that all information is correct before signing:
5. Complete the final section with the patient's printed name, signature, the date, and the name of any interpreter or translator if applicable:
Step 3: Review the completed form and click "Done." Sign up for FormsPal to download your completed authorization PDF and access it later from your account.
Common Questions About the CDCR 7385 Authorization
Who needs to use this form?
Current or former California corrections inmates, their authorized representatives, and healthcare providers use this authorization to transfer protected health information to a named person or organization outside the facility.
What types of health information can be released?
The authorization covers medical data, dental data, mental health treatment information, substance use disorder treatment files, communicable disease data, and genetic testing information. Psychotherapy notes are excluded and require a separate patient authorization under HIPAA and California law.
How long does the authorization stay valid?
The form includes a specific expiration date or expiration event set by the patient. Once that date or event occurs, the authorization is no longer valid. You can also revoke the authorization in writing at any time before health information is actually released by contacting the facility.
For other health information release documents, see our Health Information Release Form or the United Healthcare Release of Information Form.