
FormsPal provides a free online editor to complete the CDCR 1824 form directly in your browser. No downloads or special software are required. Follow the steps below to fill out and save your Reasonable Accommodation Request.
Step 1: Open the CDCR 1824 Form
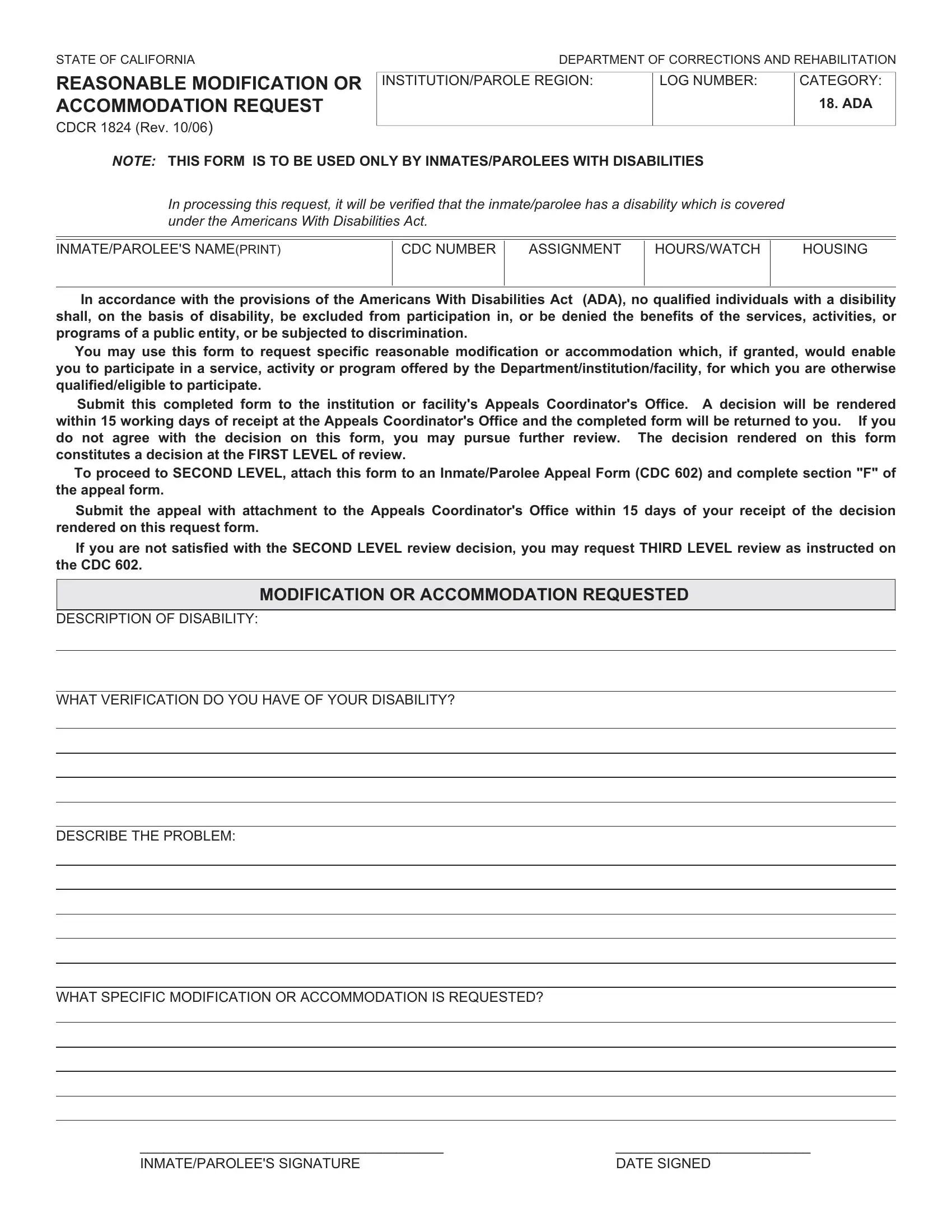
Click the "Fill Out Online" button at the top of this page to open the CDCR 1824 form in FormsPal's PDF editor. The form loads instantly in your browser.
Step 2: Enter Your Information
Complete each field in the form: your name, CDCR number, housing unit, and facility information in the personal section. In the disability section, describe how your condition limits your access to programs, work, or daily activities. Be clear and specific. In the accommodation section, describe the exact modification or aid you are requesting, such as large-print materials, a hearing amplifier, or modified seating.
Step 3: Review and Download
Review all entries for accuracy before finalizing. Click "Done" in FormsPal to save or print your completed CDCR 1824 form. Submit the printed copy to your institution's Appeals Coordinator or Correctional Counselor. Always keep a copy for your personal records.
If you need other California Department of Corrections forms, FormsPal also offers the CDCR 602 grievance form and the CDCR 7385 form.