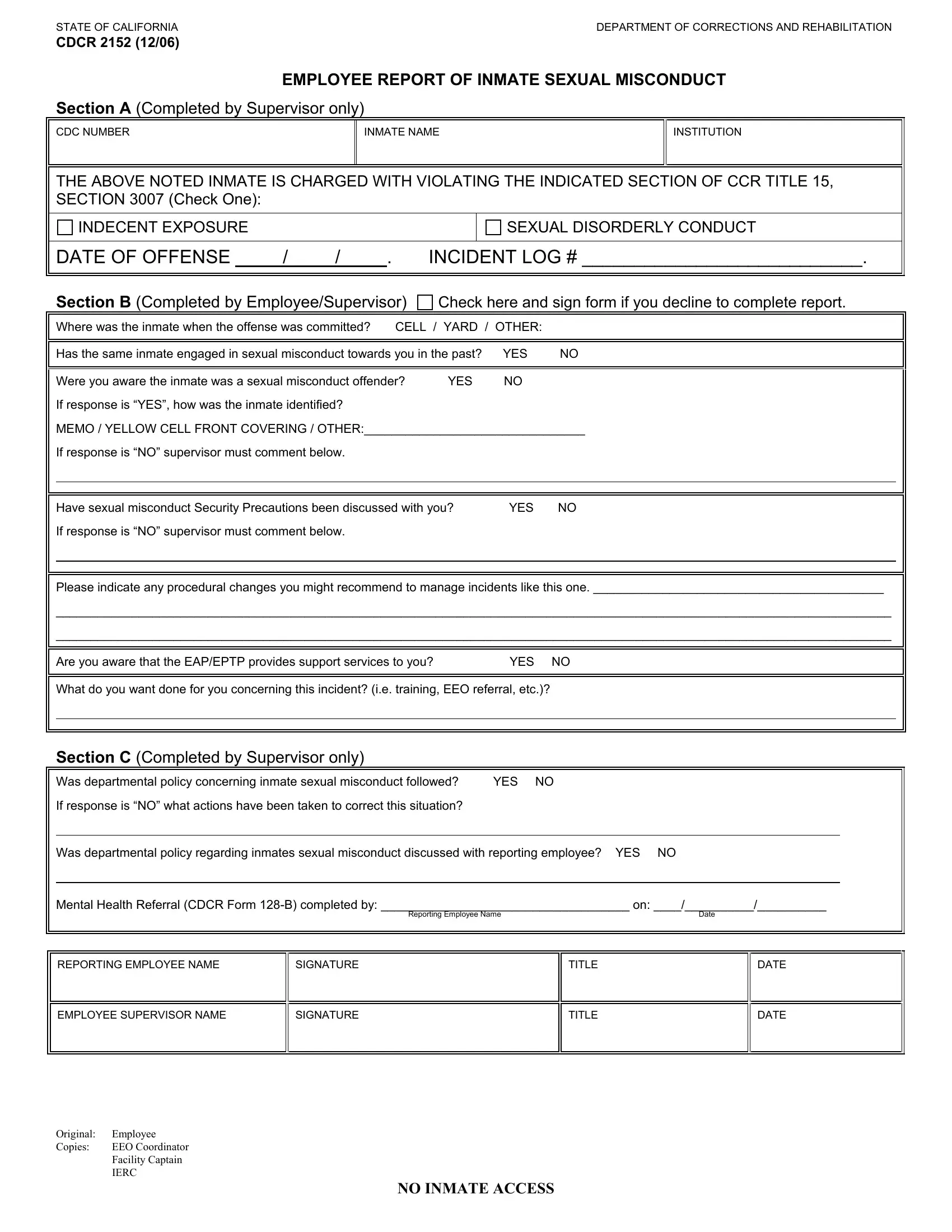
In addressing the complexities faced by employees within the correctional system, the State of California Department of Corrections and Rehabilitation has designed CDCR 2152 form, a critical document focusing on the reporting of inmate sexual misconduct. Initiated to uphold the integrity of the penal system and safeguard the well-being of its staff, this form serves as an essential tool in documenting and responding to incidents of sexual misconduct by inmates. The form is carefully structured to ensure detailed reporting, featuring sections to be completed by supervisors and the reporting employee. It captures the date of the offense, inmate information, the nature of the misconduct, and whether previous incidents involving the same inmate have occurred. Additionally, it inquires about the employee's knowledge of the inmate's history with sexual misconduct, measures discussed or taken to prevent such incidents, and recommendations for procedural changes to better handle future occurrences. Recognized protocols and support services available to employees, such as the Employee Assistance Program (EAP)/Employee Psychological Treatment Program (EPTP), are also highlighted to ensure a comprehensive support system post-reporting. Through establishing whether departmental policies were adhered to, and documenting any corrective actions taken, the CDCR 2152 form plays a pivotal role in fostering a safer work environment for corrections staff while holding inmates accountable for their behavior.
| Question | Answer |
|---|---|
| Form Name | Form Cdcr 2152 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | EPTP, california cdcr2152 pdf, IERC, california 2152 form |
