
Dealing with PDF files online is actually super easy with this PDF editor. You can fill out use cdcr only here with no trouble. FormsPal development team is continuously working to develop the tool and make it much faster for clients with its cutting-edge features. Take your experience to the next level with continually growing and unique possibilities we provide! With a few easy steps, you can begin your PDF journey:
Step 1: Click on the "Get Form" button above on this webpage to access our PDF tool.
Step 2: This tool will give you the ability to change nearly all PDF documents in a variety of ways. Enhance it by writing customized text, adjust original content, and place in a signature - all doable within a few minutes!
This document will require specific information; to guarantee correctness, please pay attention to the subsequent suggestions:
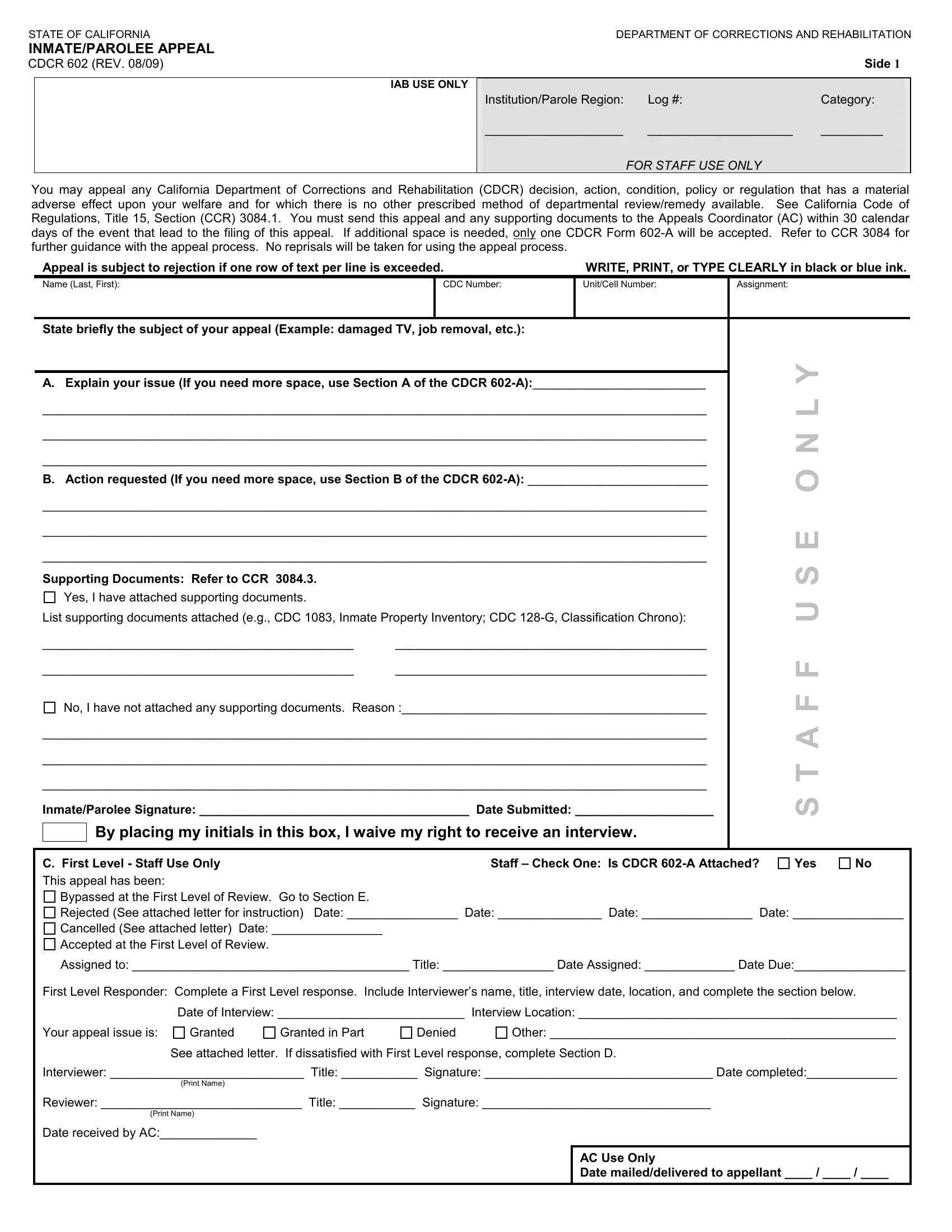
1. Whenever filling out the use cdcr only, be certain to incorporate all of the needed blanks in their corresponding form section. This will help speed up the work, allowing for your information to be processed swiftly and correctly.
2. The third step is to fill in all of the following blank fields: InmateParolee Signature Date, By placing my initials in this box, C First Level Staff Use Only This, Staff Check One Is CDCR A Attached, Yes, Bypassed at the First Level of, Assigned to Title Date Assigned, First Level Responder Complete a, Date of Interview Interview, Your appeal issue is, Granted, Granted in Part, Denied, Other, and See attached letter If.
3. This step is generally straightforward - complete all the blanks in D If you are dissatisfied with the, for processing within calendar, InmateParolee Signature Date, E Second Level Staff Use Only, Yes, This appeal has been, Bypassed at Second Level of Review, Assigned to Title Date Assigned, Second Level Responder Complete a, interview date and location and, Date of Interview Interview, Your appeal issue is, Granted, Granted in Part, and Denied in order to complete this part.
In terms of Your appeal issue is and Assigned to Title Date Assigned, be certain you review things in this section. Both these could be the key ones in the form.
4. To go onward, this section requires filling out a handful of blanks. Included in these are F If you are dissatisfied with the, InmateParolee Signature Date, G Third Level Staff Use Only, This appeal has been, Rejected See attached letter for, Other, Granted in Part, Granted, Denied, See attached Third Level response, T Third Level Use Only, Date maileddelivered to appellant, Request to Withdraw Appeal I, InmateParolee Signature Date, and Print Staff Name Title Signature, which are integral to carrying on with this process.
Step 3: Make sure your details are right and then click on "Done" to continue further. Sign up with us right now and easily gain access to use cdcr only, set for download. Each and every edit made is conveniently saved , making it possible to change the form further if necessary. FormsPal ensures your data confidentiality by using a protected method that never records or distributes any kind of sensitive information involved in the process. Be assured knowing your files are kept safe whenever you work with our service!