

You could complete dcfs physical form for adults instantly with the help of our PDFinity® PDF editor. To retain our editor on the forefront of convenience, we work to put into practice user-oriented capabilities and improvements on a regular basis. We're always looking for feedback - join us in revolutionizing the way you work with PDF documents. For anyone who is seeking to get going, here is what it will take:
Step 1: Access the PDF doc inside our editor by hitting the "Get Form Button" in the top section of this webpage.
Step 2: The editor will allow you to modify your PDF in a range of ways. Modify it by including personalized text, adjust existing content, and include a signature - all close at hand!
Pay attention while filling in this form. Ensure that all necessary blanks are done correctly.
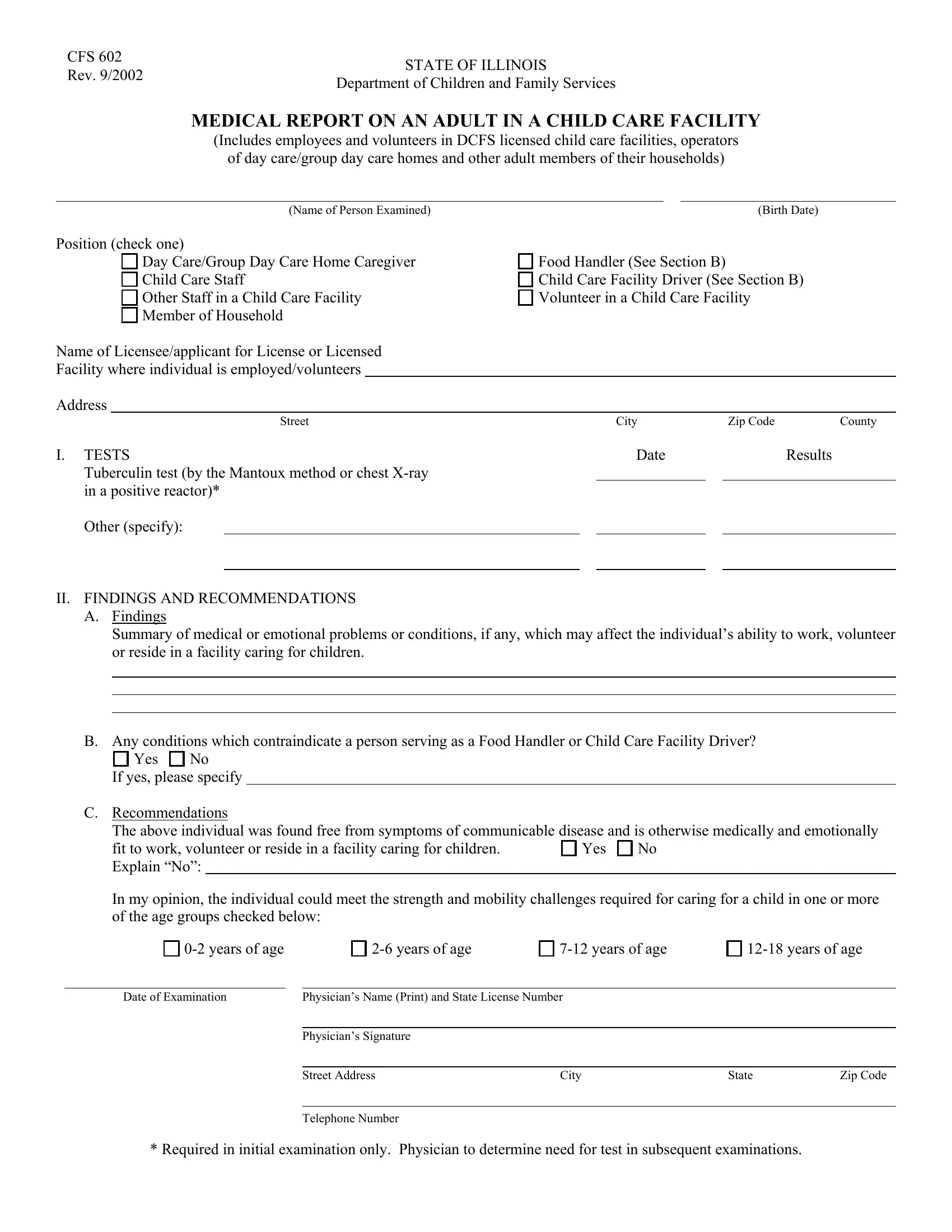
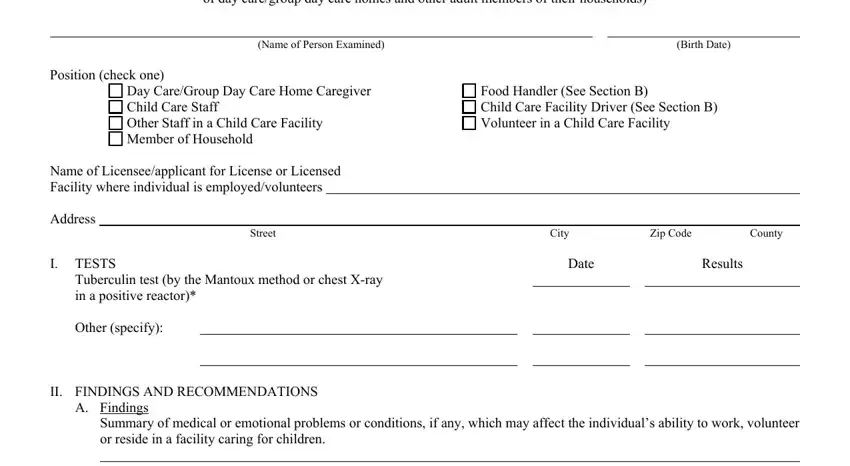
1. The dcfs physical form for adults usually requires certain information to be typed in. Ensure that the subsequent blank fields are completed:
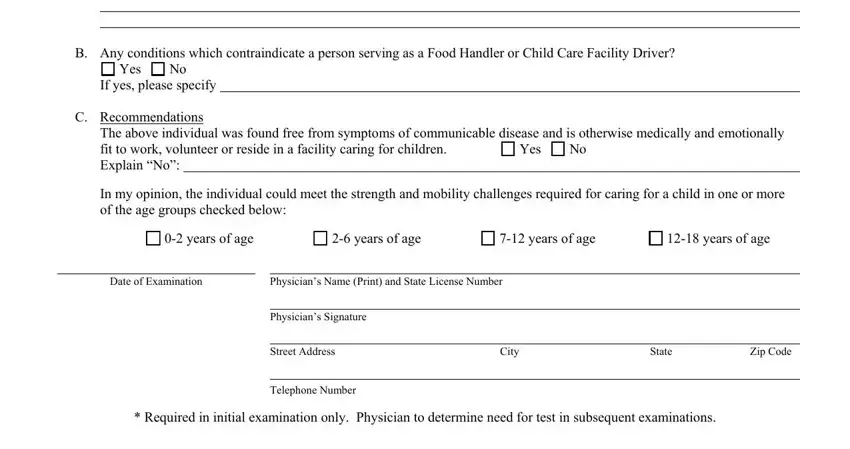
2. Once the previous segment is complete, it's time to insert the necessary particulars in Summary of medical or emotional, B Any conditions which, Yes, If yes please specify, C Recommendations, The above individual was found, Yes, years of age, years of age, years of age, years of age, Date of Examination, Physicians Name Print and State, Physicians Signature, and Street Address so you're able to proceed further.
3. This stage is simple - complete every one of the form fields in Date of Examination, Physicians Name Print and State, Date of Examination, Physicians Name Print and State, Date of Examination, and Physicians Name Print and State to complete this segment.
4. The next subsection arrives with the next few fields to consider: Date of Examination, Physicians Name Print and State, Date of Examination, and Physicians Name Print and State.
It's very easy to make a mistake when completing your Date of Examination, consequently be sure to take a second look prior to when you submit it.
5. To finish your document, the last area features a couple of additional blank fields. Entering Date of Examination, and Physicians Name Print and State should conclude everything and you can be done in an instant!
Step 3: Just after rereading your completed blanks, press "Done" and you're all set! Try a free trial option at FormsPal and acquire immediate access to dcfs physical form for adults - which you may then work with as you would like inside your FormsPal account page. FormsPal offers secure document editor with no personal data record-keeping or sharing. Be assured that your information is in good hands here!