
You could fill out cdcr form7385 instantly by using our PDFinity® online tool. The tool is continually updated by us, receiving powerful features and becoming greater. For anyone who is looking to begin, this is what it's going to take:
Step 1: Hit the "Get Form" button above. It's going to open our pdf editor so you can begin filling in your form.
Step 2: As you launch the PDF editor, you'll see the form prepared to be filled in. Besides filling out different blanks, you can also perform some other things with the form, that is adding custom words, editing the initial text, inserting graphics, signing the document, and a lot more.
Be attentive while completing this document. Ensure each and every blank field is filled out correctly.
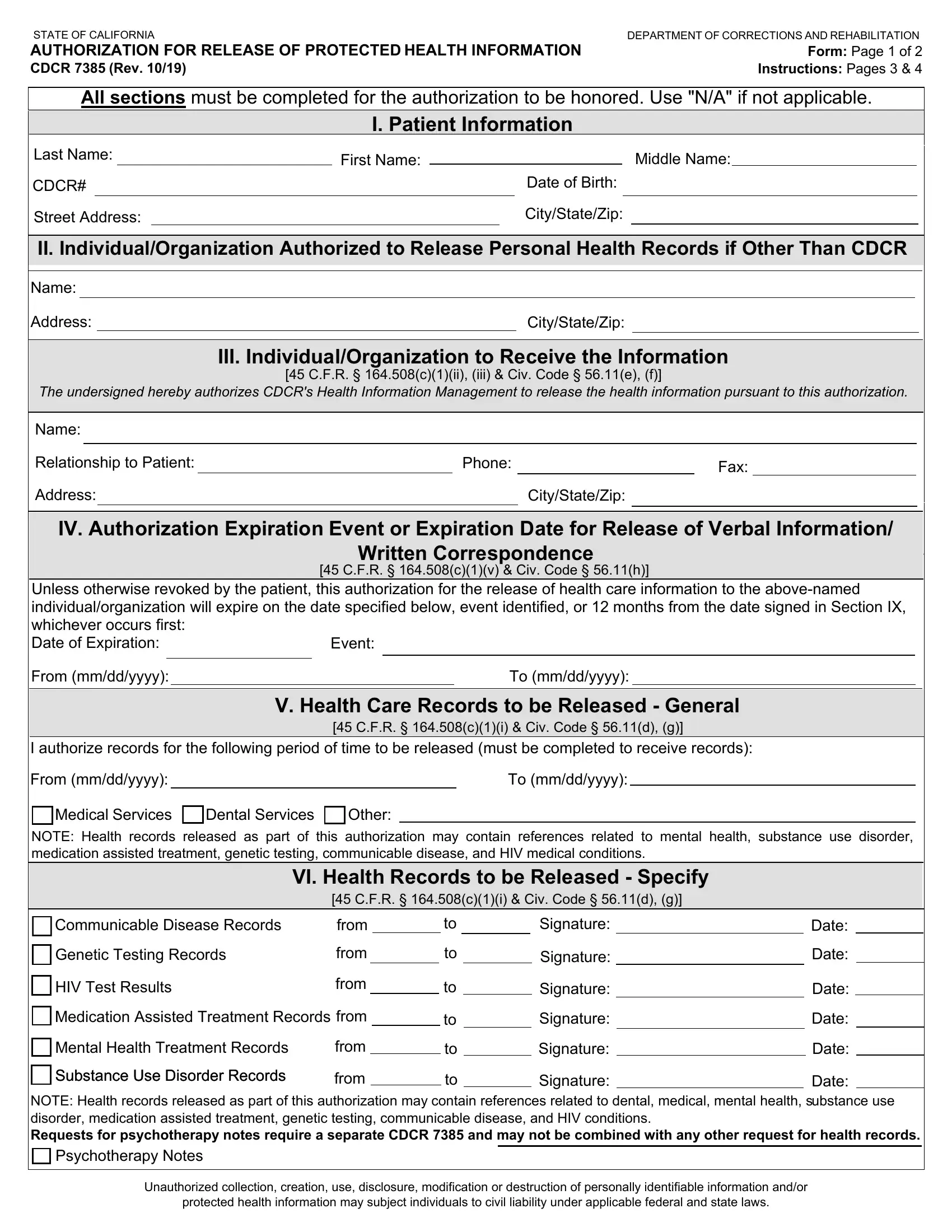
1. You will want to fill out the cdcr form7385 accurately, so be attentive while filling out the parts including all these blank fields:
2. The next part is to fill in all of the following fields: Unless otherwise revoked by the, Event, From mmddyyyy, V Health Care Records to be, CFR ci Civ Code d g, To mmddyyyy, I authorize records for the, From mmddyyyy, To mmddyyyy, Medical Services, Dental Services, Other, NOTE Health records released as, VI Health Records to be Released, and Communicable Disease Records.
Those who work with this document generally make mistakes while completing CFR ci Civ Code d g in this part. Make sure you go over whatever you type in here.
3. In this part, examine NOTE Health records released as, Psychotherapy Notes, Unauthorized collection creation, and protected health information may. All of these have to be taken care of with greatest awareness of detail.

4. Filling in Health Care, Personal Use, Legal, VII Purpose for the Release or Use, CFR civ Other please specify, VIII Authorization Information, I understand the following I, I have the right to revoke this, I am signing this authorization, Under California law the, and If the organization or person I is key in the next part - always spend some time and fill out every single blank area!
5. And finally, the following final part is what you'll want to complete before finalizing the PDF. The fields under consideration include the following: CFR cvi Civ Code c, Name Print, Signature If no expiration date is, Date, Name of person signing form if not, Date, Name of translatorinterpreter, Signature of translatorinterpreter, Date Unauthorized collection, and protected health information may.
Step 3: Right after you've reviewed the information you filled in, press "Done" to conclude your form. Grab your cdcr form7385 once you sign up at FormsPal for a 7-day free trial. Instantly get access to the pdf within your FormsPal cabinet, along with any modifications and changes being conveniently synced! At FormsPal.com, we endeavor to be sure that all of your information is stored protected.