
The CEM-2501 form is straightforward to complete when you know what each section requires. This guide explains who must file it, when to submit it, and how to fill out every field correctly the first time.
What Is the CEM-2501 Fringe Benefit Statement?
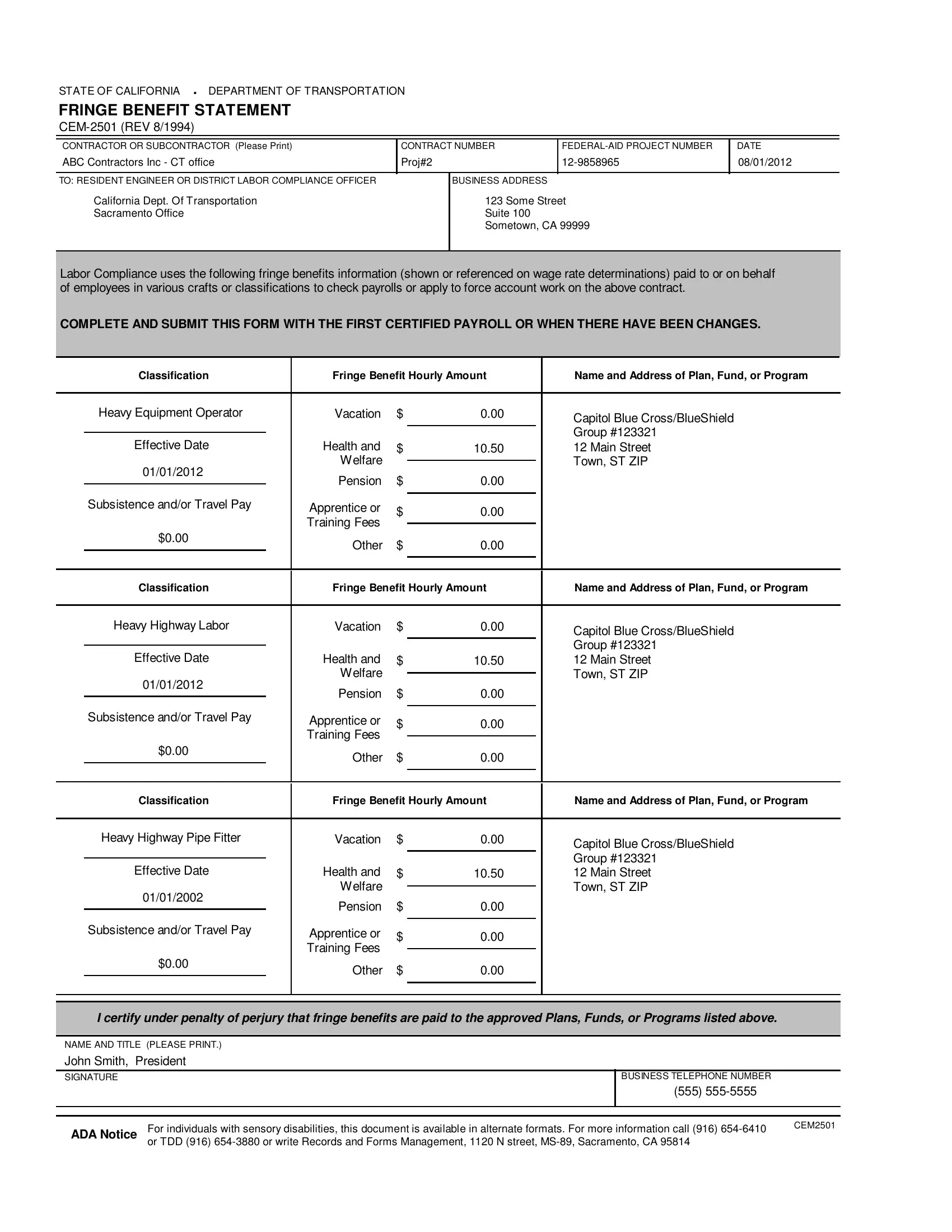
The CEM-2501 is a state document issued by the California Department of Transportation, known as Caltrans. Contractors and subcontractors use it to record and disclose the fringe benefits they provide to workers on federal-aid highway and bridge projects. The form captures dollar amounts paid per hour for six categories of benefits: health and welfare, pension, vacation, subsistence, travel pay, and apprenticeship or training fees. Labor compliance officers and resident engineers check these numbers against certified payroll records to confirm workers receive the full benefit package required by the prevailing wage determination.
Who Needs to File the CEM-2501 Form?
Any contractor or subcontractor that employs workers on a Caltrans federal-aid construction contract must file a CEM-2501. This includes general contractors, prime subcontractors, and lower-tier subcontractors at every level of the project workforce. Each company files its own form. A CEM-2501 submitted by the prime contractor does not cover benefits paid by a subcontractor. Every company in the contracting chain is responsible for its own disclosure.
When Do You Need to Submit the CEM-2501?
Submit the CEM-2501 together with your first certified payroll for the contract. If your benefit amounts change at any time during the project, submit a revised form before the next payroll period closes. Waiting until a payroll audit to correct benefit figures can result in a Notice of Non-Compliance, which puts progress payments on hold until Caltrans accepts the corrected documentation.
How to Fill Out the CEM-2501 Form: Step-by-Step Guide
Follow these steps to complete the CEM-2501 correctly:
- Enter the contract identification details. Write the Caltrans contract number, the county, and the route or highway at the top of the form. These three fields tie your benefit disclosure to a specific project record.
- Provide your company information. Enter the name of the contractor or subcontractor, the business address, and the contractor license number. Every company on the project files separately, so your identifying information must be accurate.
- List each job classification. Write the name of each trade or craft that your company employs on the project. Common classifications include Laborer, Carpenter, Ironworker, Operating Engineer, and Teamster. Workers who receive identical benefit packages can be grouped under one classification row.
- Record the hourly benefit amounts. For each classification, fill in the hourly dollar amount for each of the six fringe benefit categories. Use the applicable Davis-Bacon or California prevailing wage determination as your reference. Do not estimate or round the figures.
- Identify each benefit plan or fund. In the plan identification column, name the specific trust fund, insurance carrier, or program that provides each benefit. Include fund identification numbers when the determination or the plan document requires them. For cash equivalents paid directly to workers, write "cash equivalent" in this column.
- Calculate the total hourly benefit. Add all six categories for each classification to arrive at the total fringe benefit amount per hour. This total must match the fringe benefit line shown on your certified payroll records for that classification.
- Sign and date the form. An authorized representative, such as the project manager or owner, must sign and date the completed form. An unsigned form is incomplete and will be returned.
What Fringe Benefits Are Listed on the CEM-2501?
The form covers six categories of fringe benefits recognized under federal and California prevailing wage rules:
- Health and welfare includes medical, dental, and vision insurance premiums paid by the employer on behalf of the worker.
- Pension refers to employer contributions to retirement savings plans, annuities, or other deferred compensation programs.
- Vacation covers paid time off accrued by the worker, expressed as an hourly dollar equivalent.
- Subsistence is a daily or hourly allowance paid when a worker must temporarily relocate to reach a distant job site.
- Travel pay compensates workers for the cost of traveling to and from the project site when the site is beyond the local area covered by the applicable wage determination.
- Apprenticeship and training fees fund registered apprenticeship programs. Contractors direct these amounts to the sponsoring program trust fund.
Tips for Completing the CEM-2501 Without Errors
Gather your prevailing wage determinations, union collective bargaining agreements, and trust fund contribution rates before you open the form. Inconsistencies between these source documents and the amounts you enter are the main cause of labor compliance audits. Compare your CEM-2501 figures against the fringe benefit line on each certified payroll submission before you hand both documents to the resident engineer. If a plan changes its contribution rate mid-project, note the effective date on the revised CEM-2501 so the compliance officer can trace the change to a specific payroll period.
Frequently Asked Questions
Does each subcontractor file its own CEM-2501?
Yes. Every company that employs workers on the project must submit a separate form. The prime contractor's CEM-2501 does not cover benefits paid by a subcontractor.
Can a contractor pay a cash equivalent instead of providing a benefit plan?
California prevailing wage law generally allows cash equivalents for some benefit categories when the applicable wage determination permits it. Note "cash equivalent" in the plan identification column and verify that cash payment is consistent with the determination for your project.
How long must I keep CEM-2501 records after the project ends?
California labor regulations require contractors to retain payroll and benefit records for at least three years after project completion. Keep your signed CEM-2501 forms with the certified payroll records for the same contract.
What happens if I submit incorrect benefit amounts?
The resident engineer or labor compliance officer may issue a Notice of Non-Compliance. You will need to resubmit corrected forms and adjust worker payments for any period of underpayment. Repeated violations can restrict your ability to bid on future state-funded construction work.
Who reviews the CEM-2501 after submission?
Caltrans labor compliance officers and resident engineers review the form. They cross-check the hourly benefit amounts against your certified payroll records and the prevailing wage determination for the contract.
Related Forms for Construction Contractors
Contractors on public works projects typically need several documents alongside the CEM-2501. A certified payroll form records weekly wages and hours for each worker on a federal-aid project. A subcontractor agreement defines the scope, timeline, and payment terms between the prime contractor and its subs. A construction proposal form documents bid details before work begins.