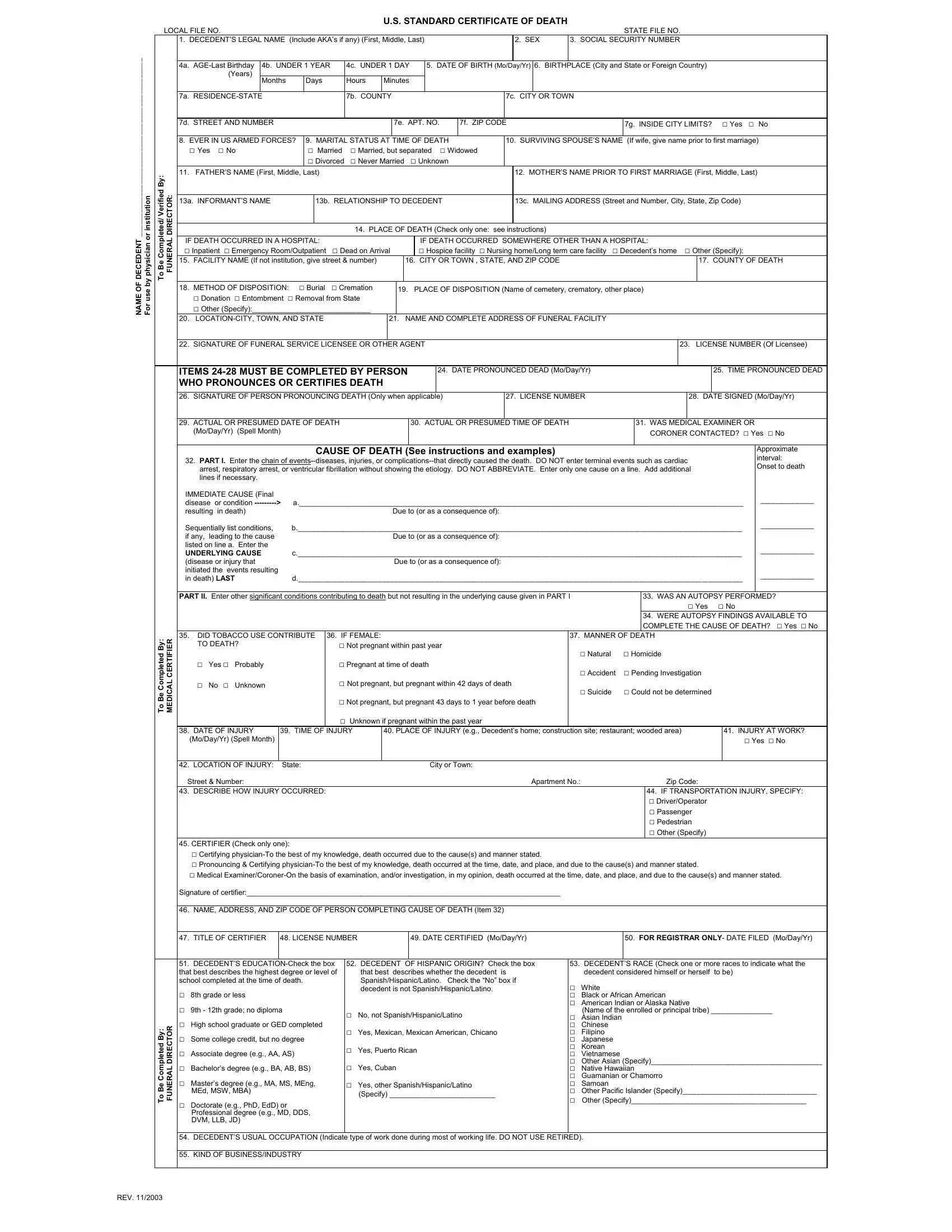
When a life comes to an end, a series of formal steps must be taken to legally acknowledge the death, one of which involves the completion of the U.S. Standard Certificate of Death. This document, a crucial part of the process, is filled out by either a physician or an institution. It captures detailed information about the deceased, such as their legal name, including any known aliases, gender, social security number, age, date and place of birth, and residence. It goes further to record aspects of their life, including military service, marital status, and educational attainment. The form also delves into the medical cause of death, listing the immediate cause and any underlying causes sequentially, and inquires about autopsy performance and its findings, tobacco use contribution, and the manner of death. Details regarding the place and time of death, as well as the method and location of disposition, are meticulously noted. Furthermore, the form gathers information about the informant, the person pronouncing death, and the certifier, ensuring a comprehensive record. The meticulous documentation required underscores the significance of this form in not only providing closure to the bereaved but also serving a legal and statistical role in society.
| Question | Answer |
|---|---|
| Form Name | Certification Death Form |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | printable death certificates, how certificate death form download, death certification form, when certificate death form download |