
Any time you desire to fill out csf meaning philhealth, you won't have to install any software - just give a try to our online tool. To have our tool on the cutting edge of efficiency, we strive to put into practice user-oriented features and enhancements on a regular basis. We're at all times thankful for any suggestions - assist us with revampimg PDF editing. Getting underway is easy! Everything you need to do is stick to these easy steps directly below:
Step 1: Simply click on the "Get Form Button" in the top section of this site to start up our pdf form editing tool. This way, you'll find all that is required to fill out your file.
Step 2: With the help of our online PDF editor, you can accomplish more than merely fill out forms. Try each of the functions and make your forms look professional with custom text added, or optimize the file's original input to excellence - all that supported by the capability to insert stunning graphics and sign the document off.
This form will need you to provide specific details; to guarantee accuracy, please be sure to consider the guidelines just below:
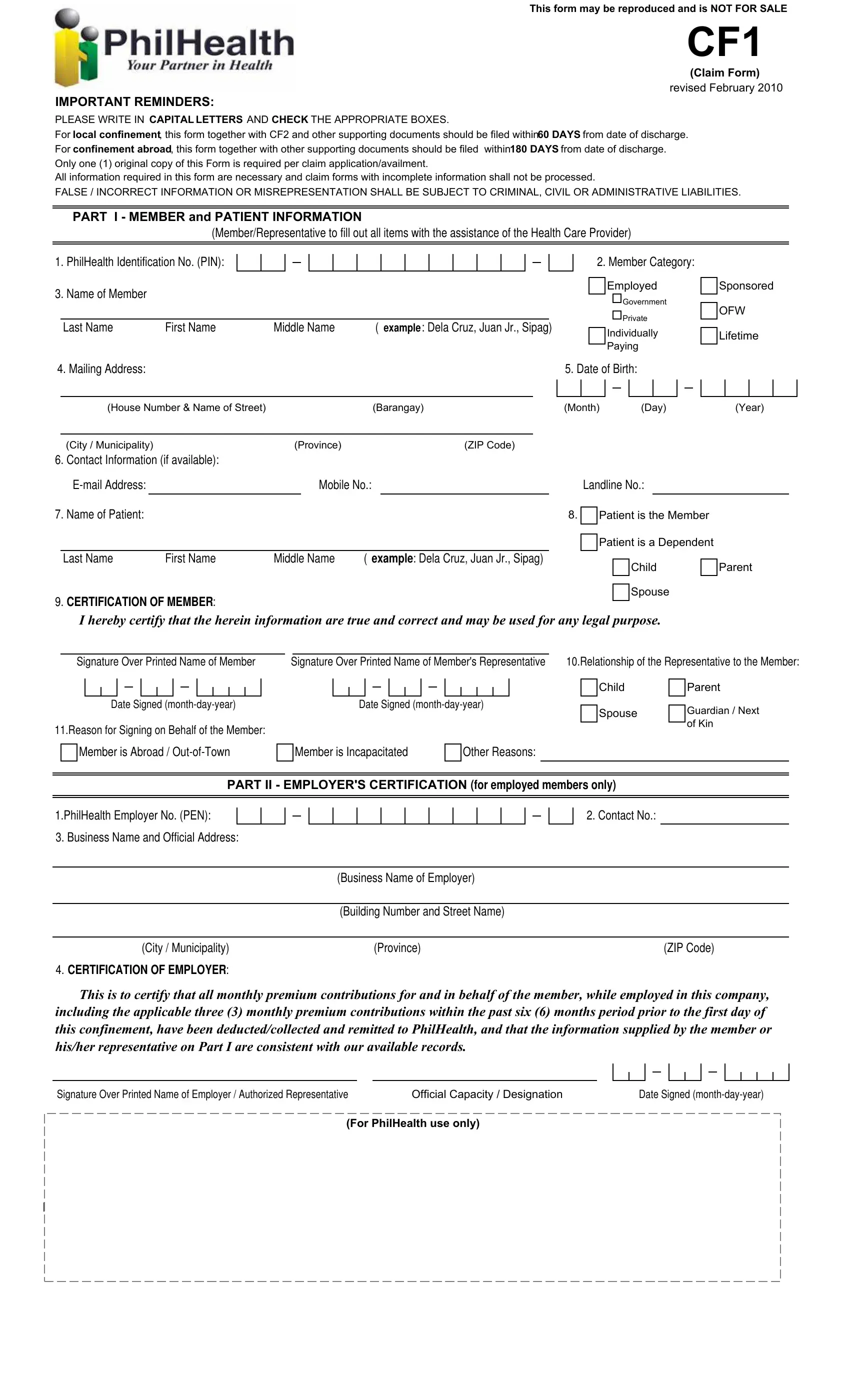
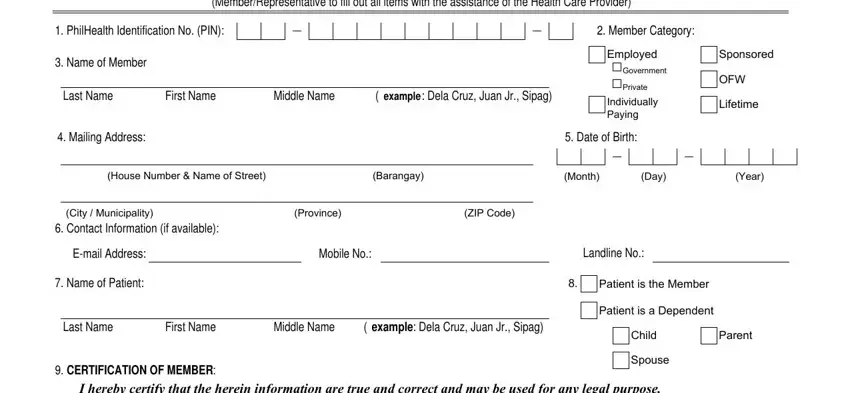
1. To begin with, once completing the csf meaning philhealth, beging with the section that contains the next fields:
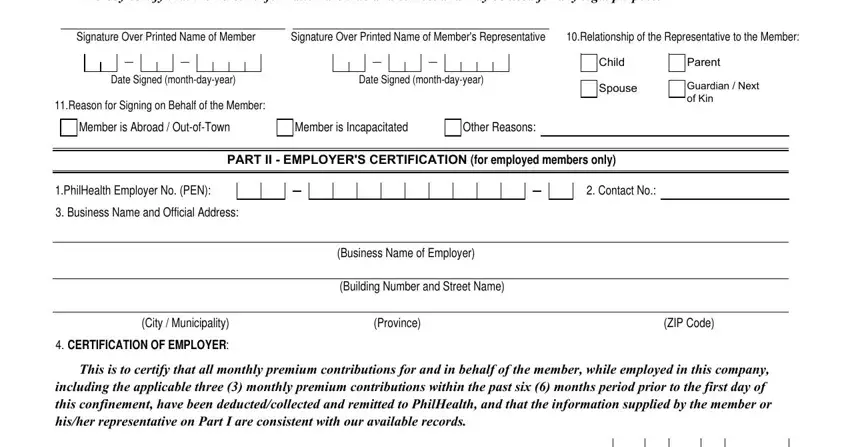
2. The next stage is usually to fill out these particular blank fields: I hereby certify that the herein, Signature Over Printed Name of, Signature Over Printed Name of, Relationship of the Representative, Date Signed monthdayyear, Date Signed monthdayyear, Reason for Signing on Behalf of, Member is Abroad OutofTown, Member is Incapacitated, Other Reasons, Child, Parent, Spouse, Guardian Next of Kin, and PART II EMPLOYERS CERTIFICATION.
3. Completing For PhilHealth use only is essential for the next step, make sure to fill them out in their entirety. Don't miss any details!
Be really mindful when filling out For PhilHealth use only and For PhilHealth use only, since this is the part where a lot of people make some mistakes.
Step 3: Confirm that the details are correct and press "Done" to complete the task. Grab your csf meaning philhealth once you join for a free trial. Conveniently view the document inside your FormsPal cabinet, with any edits and changes all preserved! Whenever you work with FormsPal, you can easily fill out documents without the need to worry about database breaches or records getting distributed. Our protected system makes sure that your private data is kept safely.