

philhealth member registration form can be filled out online in no time. Just make use of FormsPal PDF editing tool to accomplish the job quickly. FormsPal development team is constantly working to expand the editor and enable it to be much easier for clients with its extensive functions. Bring your experience to the next level with continually improving and great options we offer! Getting underway is simple! All you have to do is adhere to these easy steps below:
Step 1: Firstly, access the tool by clicking the "Get Form Button" in the top section of this site.
Step 2: After you start the online editor, you will find the form made ready to be filled in. Other than filling in different fields, it's also possible to perform many other actions with the form, such as putting on custom text, editing the initial textual content, inserting graphics, affixing your signature to the PDF, and much more.
It is simple to finish the document using this practical guide! This is what you have to do:
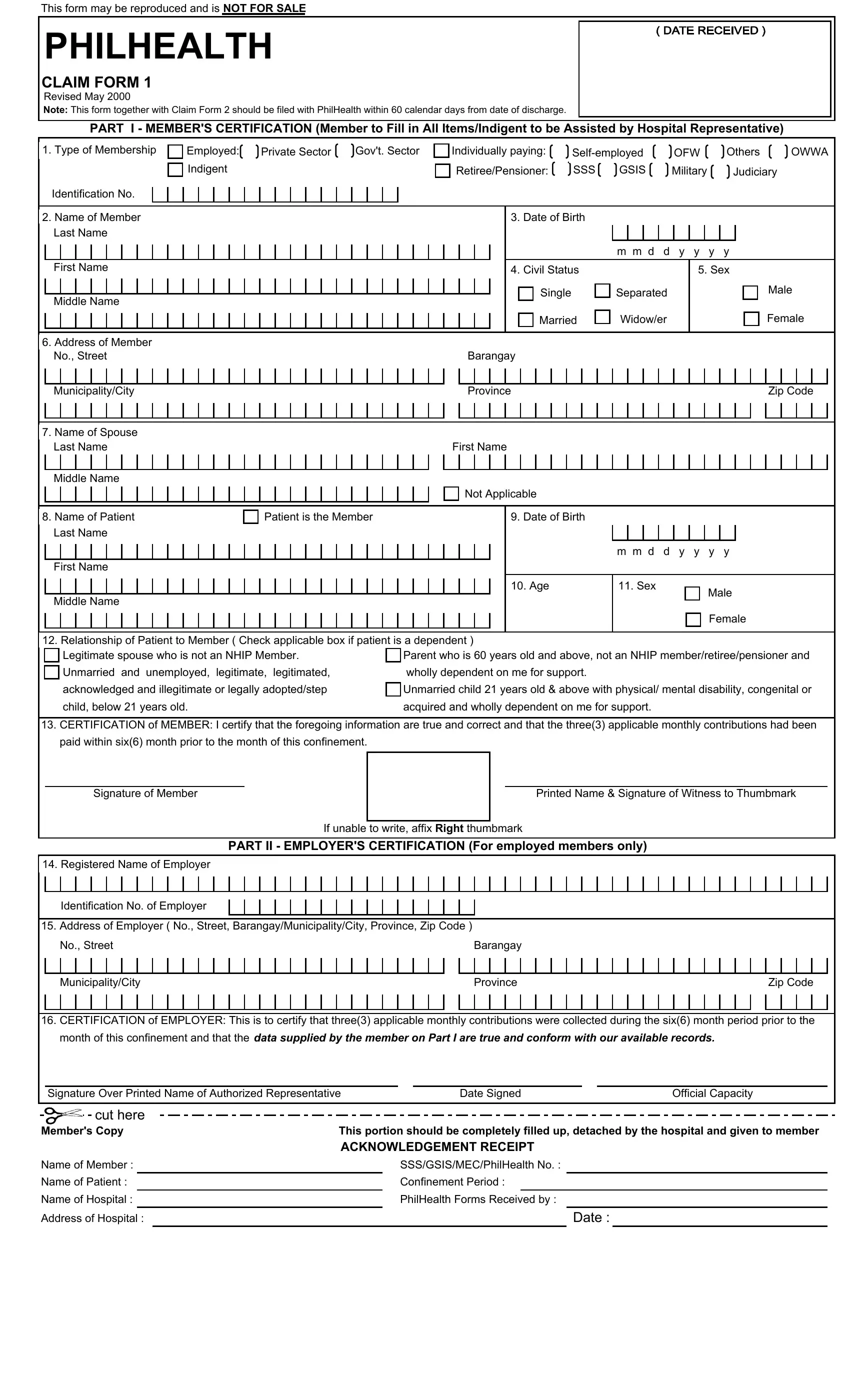
1. Fill out your philhealth member registration form with a number of major fields. Gather all the necessary information and make certain nothing is missed!
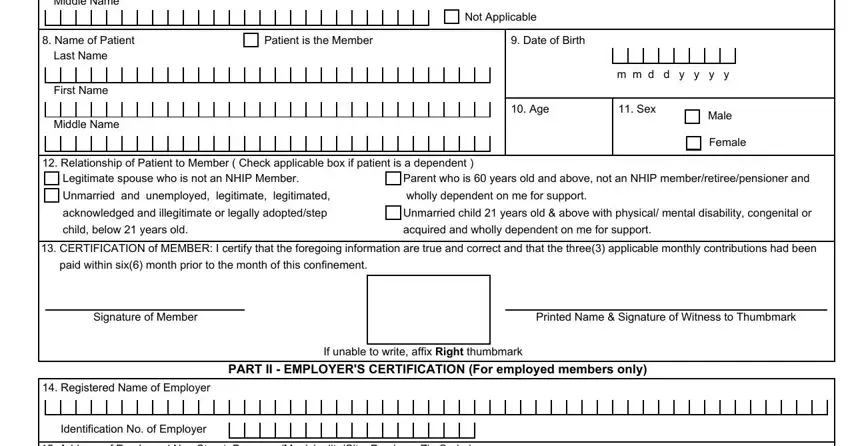
2. The subsequent stage is to complete these particular blanks: Middle Name, Name of Patient, Last Name, First Name, Middle Name, Not Applicable, Patient is the Member, Date of Birth, m m d d y y y y, Age, Sex, Male, Female, Relationship of Patient to Member, and Legitimate spouse who is not an.
3. This next part is related to No Street, MunicipalityCity, Barangay, Province, Zip Code, CERTIFICATION of EMPLOYER This is, month of this confinement and that, Signature Over Printed Name of, Date Signed, Official Capacity, cut here, Members Copy, Name of Member, Name of Patient, and Name of Hospital - complete these empty form fields.
You can potentially make errors while filling out your cut here, and so ensure that you look again before you decide to send it in.
Step 3: Proofread the details you've inserted in the form fields and click the "Done" button. After setting up a7-day free trial account at FormsPal, you'll be able to download philhealth member registration form or send it through email promptly. The PDF file will also be available from your personal cabinet with all of your edits. FormsPal guarantees secure form editor without personal data recording or any sort of sharing. Feel comfortable knowing that your details are safe here!