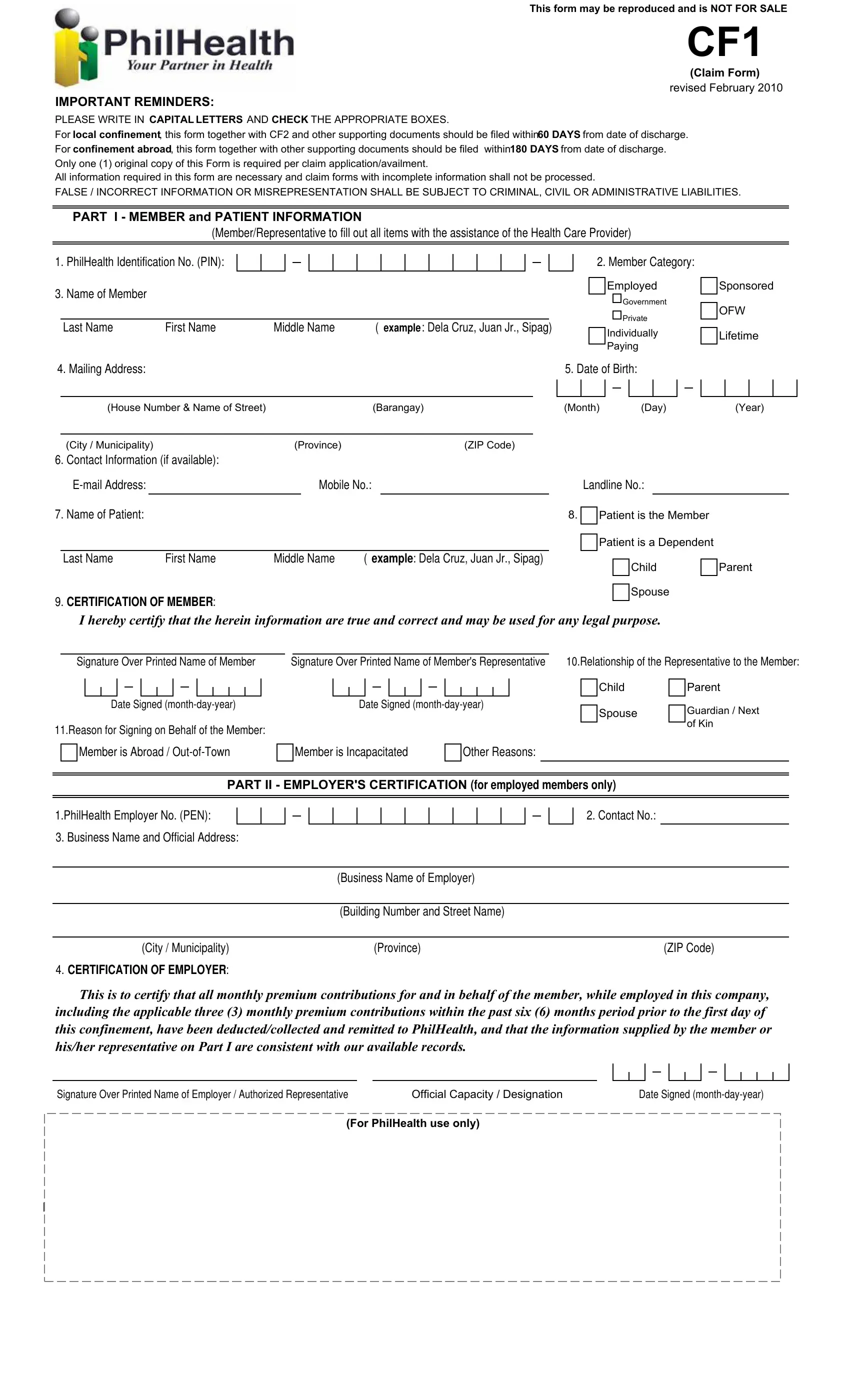
The CF1 PhilHealth form, revised in September 2018, is the official Claim Form 1 issued by the Philippine Health Insurance Corporation (PhilHealth). Members use this form to file claims for inpatient and outpatient health benefits covered under the National Health Insurance Program. The form must be completed using CAPITAL letters, with all relevant boxes ticked to prevent processing delays.
Any PhilHealth member, or their authorized representative, must file the CF1 form when claiming health insurance benefits after a hospital confinement or qualifying outpatient procedure. Employed members, voluntary contributors, overseas Filipino workers (OFWs), and sponsored members can all use this form. The member's employer must certify that premium contributions are current for employed individuals.
The CF1 PhilHealth form contains five main parts. Part I collects member and patient information, including the PhilHealth Identification Number (PIN), member category, and contact details. Part II is the employer's certification for employed members, confirming that contributions have been paid. Part III covers the member or representative certification, where the filer attests to the accuracy of all provided information. Part IV handles authorization for a representative to sign on behalf of the member when the member is abroad, incapacitated, or otherwise unable to file in person. Part V is reserved for PhilHealth office use during claims processing.
For local hospital confinements, the CF1 form and all supporting documents must be submitted within 60 calendar days from the date of discharge. For confinements abroad, the filing window extends to 180 calendar days. Only one original copy of the CF1 form is needed per claim. Submitting false or incorrect information on the form may result in criminal, civil, or administrative penalties under Philippine law.
The CF1 form is part of a set of documents required for a complete PhilHealth claim. The CF2 PhilHealth form (Claim Form 2) must be accomplished by the attending physician and submitted alongside the CF1. Members who need to register for the first time can use the PhilHealth Member Registration Form. For employer remittance records, the PhilHealth ER2 form documents premium payment details. Additionally, the PhilHealth Payment Form is used for voluntary and self-employed premium contributions.
| Question | Answer |
|---|---|
| Form Name | CF-1 Philhealth Form (Claim Form 1) |
| Form Length | 1 pages |
| Fillable? | Yes |
| Fillable fields | 76 |
| Avg. time to fill out | 15 min 31 sec |
| Other names | cf1 series of 2018, csf philhealth, how to fill up philhealth form cf1, get cf1 |