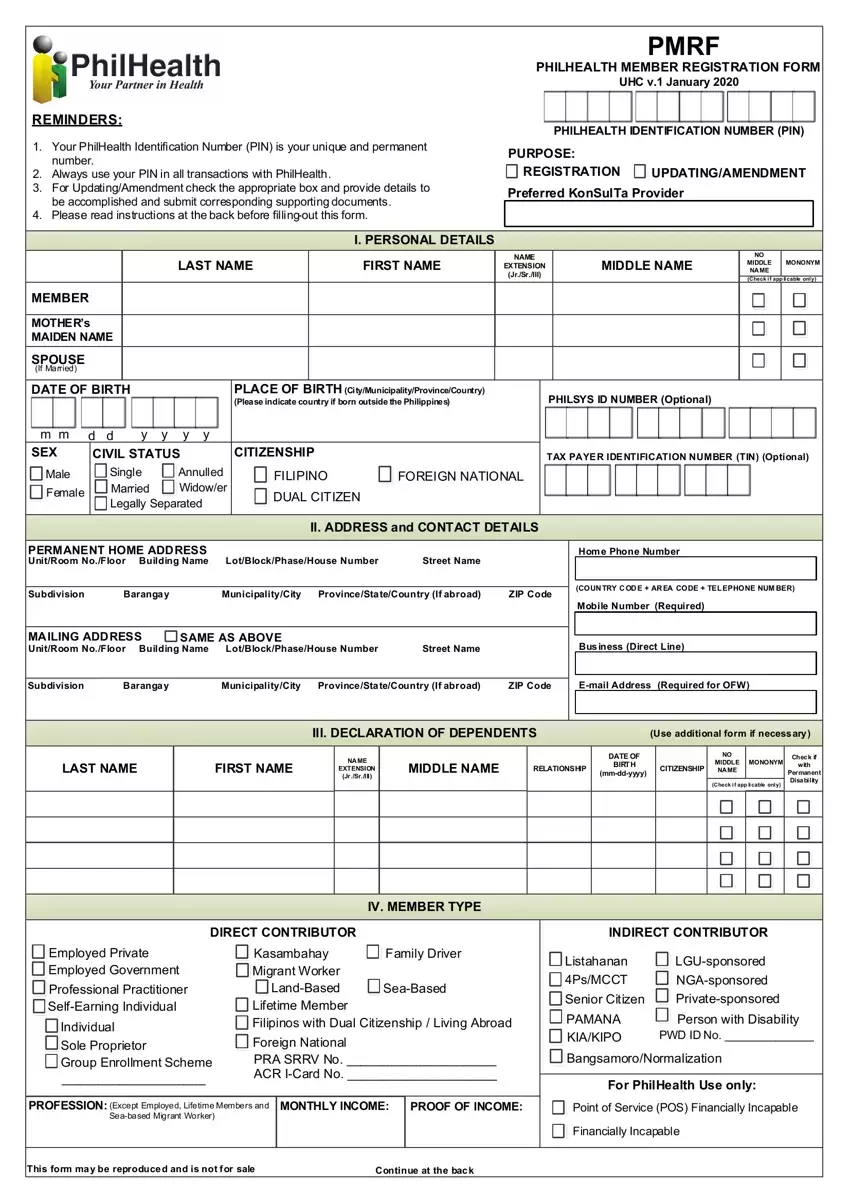
In the realm of healthcare registration in the Philippines, the PhilHealth Member Registration Form (PMRF) January 2020 version stands as a crucial document for both new enrollees and existing members seeking to update their information. This form, integral to accessing health insurance benefits under the Universal Health Care (UHC) system, demands careful attention to several key aspects. Individuals are reminded of the importance of their unique and permanent PhilHealth Identification Number (PIN), which must be used in all transactions with PhilHealth. The form caters to a variety of purposes, including registration, updating, and amendment of member details, underscoring the necessity of providing accurate personal information, preferred KonSulTa provider, dependent declarations, and specifying the member type. It is designed to capture comprehensive personal and contact details, from full names and birth details to addresses and contact numbers, ensuring coverage for a wide demographic, including direct contributors like employed individuals, migrant workers, professionals, and indirect contributors such as senior citizens and persons with disability (PWD). Furthermore, the PMRF includes instructions for the declaration of dependents, emphasizing the inclusion of children below 21 years old, the spouse, and parents above 60 years old who are wholly dependent on the member. The form also accommodates individuals with permanent disabilities, reflecting the inclusivity of the PhilHealth program. Through maintaining accurate records and adhering to the form’s guidelines, members can ensure smoother interactions with PhilHealth, facilitating access to essential healthcare services and benefits.
| Question | Answer |
|---|---|
| Form Name | Philhealth Registration Form |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | philhealth member registration form, philhealth online registration 2020, philhealth gov ph online, pmrf |
