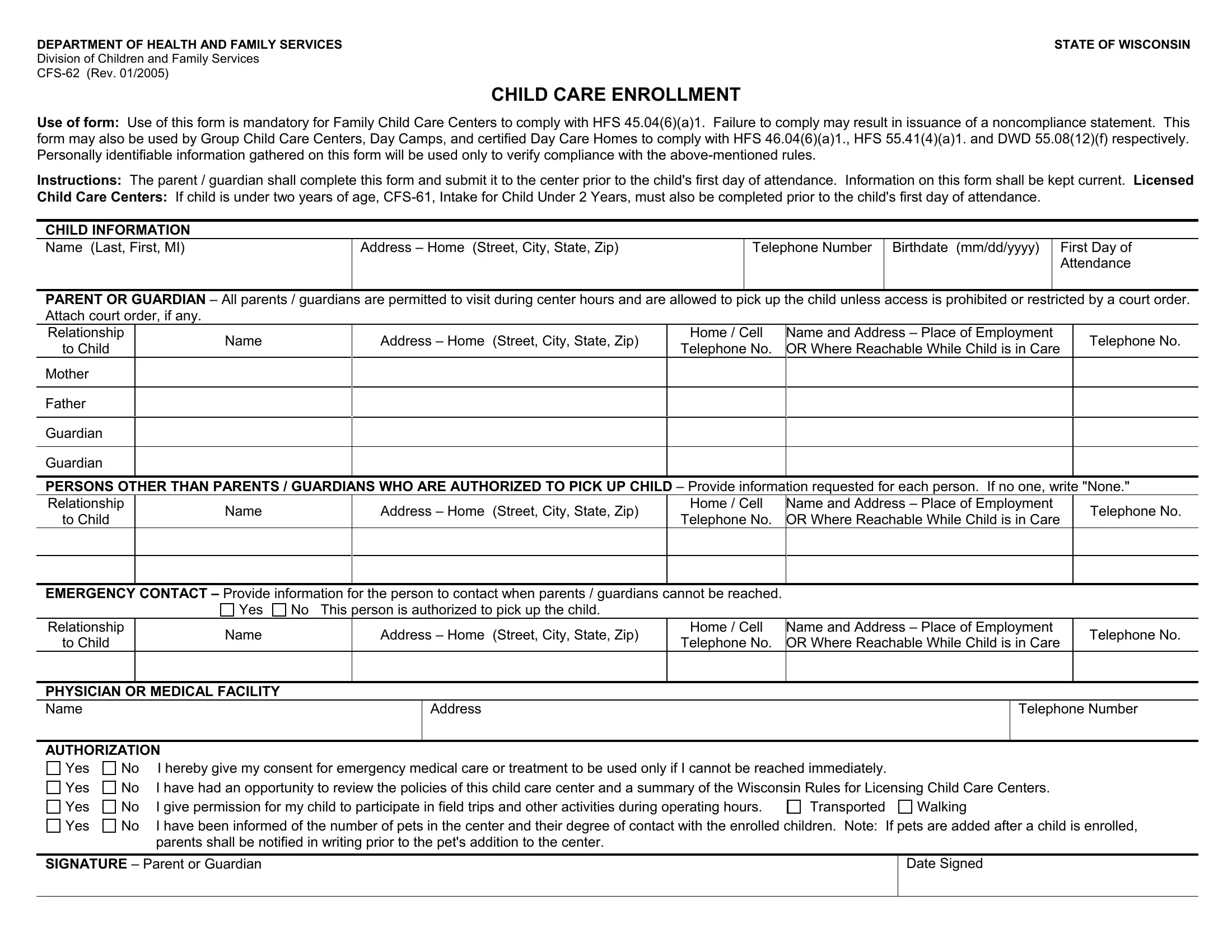
Ensuring the well-being and safety of children in child care settings is a critical responsibility, one that is facilitated by forms like the CFS-62. Issued by the Wisconsin Department of Health and Family Services, Division of Children and Family Services, the CFS-62 form, revised in January 2005, plays a pivotal role in the enrollment process of children into family child care centers, group child care centers, day camps, and certified day care homes. Its primary use, mandated to comply with several state regulations, underscores its importance in verifying adherence to specific health and safety standards. By filling out the CFS-62 form, parents or guardians provide essential information about the child’s health, emergency contacts, and persons authorized to pick up the child, ensuring clear communication and preparedness for any situation that may arise during the child's time at the center. It also includes sections for parental permissions regarding medical treatment, participation in activities, and interactions with pets in the care environment. The necessity of this form before a child's first day illustrates a proactive approach to child care, requiring that all pertinent data is collected and kept current, thereby ensuring that child care providers are well-informed and prepared to offer a safe and nurturing environment.
| Question | Answer |
|---|---|
| Form Name | Cfs 62 Form |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | ChildCareEnroll ment cfs 62 child care enrollment form |
DEPARTMENT OF HEALTH AND FAMILY SERVICES |
STATE OF WISCONSIN |
Division of Children and Family Services |
|
|
CHILD CARE ENROLLMENT
USE OF FORM: Use of this form is mandatory for Family Child Care Centers to comply with HFS 45.04(6)(a)1. Failure to comply may result in issuance of a noncompliance statement. This form may also be used by Group Child Care Centers, Day Camps, and certified Day Care Homes to comply with HFS 46.04(6)(a)1., HFS 55.41(4)(a)1. and DWD 55.08(12)(f) respectively. Personally identifiable information gathered on this form will be used only to verify compliance with the
INSTRUCTIONS: The parent / guardian shall complete this form and submit it to the center prior to the child's first day of attendance. Information on this form shall be kept current. LICENSED
CHILD CARE CENTERS: If child is under two years of age,
CHILD INFORMATION
Name (Last, First, MI) |
Address – Home (Street, City, State, Zip) |
Telephone Number |
Birthdate (mm/dd/yyyy) |
First Day of |
|
|
|
|
Attendance |
|
|
|
|
|
PARENT OR GUARDIAN – All parents / guardians are permitted to visit during center hours and are allowed to pick up the child unless access is prohibited or restricted by a court order. Attach court order, if any.
Relationship |
Name |
Address – Home (Street, City, State, Zip) |
Home / Cell |
Name and Address – Place of Employment |
Telephone No. |
|
to Child |
Telephone No. |
OR Where Reachable While Child is in Care |
||||
|
|
|
||||
Mother |
|
|
|
|
|
|
|
|
|
|
|
|
|
Father |
|
|
|
|
|
|
|
|
|
|
|
|
|
Guardian |
|
|
|
|
|
|
|
|
|
|
|
|
|
Guardian |
|
|
|
|
|
|
|
|
|
|
|
|
PERSONS OTHER THAN PARENTS / GUARDIANS WHO ARE AUTHORIZED TO PICK UP CHILD – Provide information requested for each person. If no one, write "None."
Relationship |
Name |
|
Address – Home |
(Street, City, State, Zip) |
Home / Cell |
Name and Address – Place of Employment |
Telephone No. |
||
to Child |
|
Telephone No. |
OR Where Reachable While Child is in Care |
||||||
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
||
EMERGENCY CONTACT – Provide information for the person to contact when parents / guardians cannot be reached. |
|
|
|
||||||
|
Yes |
No This person is authorized to pick up the child. |
|
|
|
|
|||
Relationship |
Name |
|
Address – Home |
(Street, City, State, Zip) |
Home / Cell |
Name and Address – Place of Employment |
Telephone No. |
||
to Child |
|
Telephone No. |
OR Where Reachable While Child is in Care |
||||||
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
PHYSICIAN OR MEDICAL FACILITY |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Name |
|
|
|
Address |
|
|
|
Telephone Number |
|
|
|
|
|
|
|
|
|
|
|
AUTHORIZATION
Yes
Yes
Yes
Yes
No |
I hereby give my consent for emergency medical care or treatment to be used only if I cannot be reached immediately. |
|
|
No |
I have had an opportunity to review the policies of this child care center and a summary of the Wisconsin Rules for Licensing Child Care Centers. |
||
No |
I give permission for my child to participate in field trips and other activities during operating hours. |
Transported |
Walking |
No |
I have been informed of the number of pets in the center and their degree of contact with the enrolled children. Note: If pets are added after a child is enrolled, |
||
|
parents shall be notified in writing prior to the pet's addition to the center. |
|
|
SIGNATURE – Parent or Guardian
Date Signed