
The CFS 431-A form, also called the DCFS psychotropic medication request form, is a required Illinois DCFS document that authorizes psychotropic medication for children in foster care and residential placements. Use FormsPal's free PDF editor to complete and download this form at no cost.
What is the CFS 431-A Form Used For?
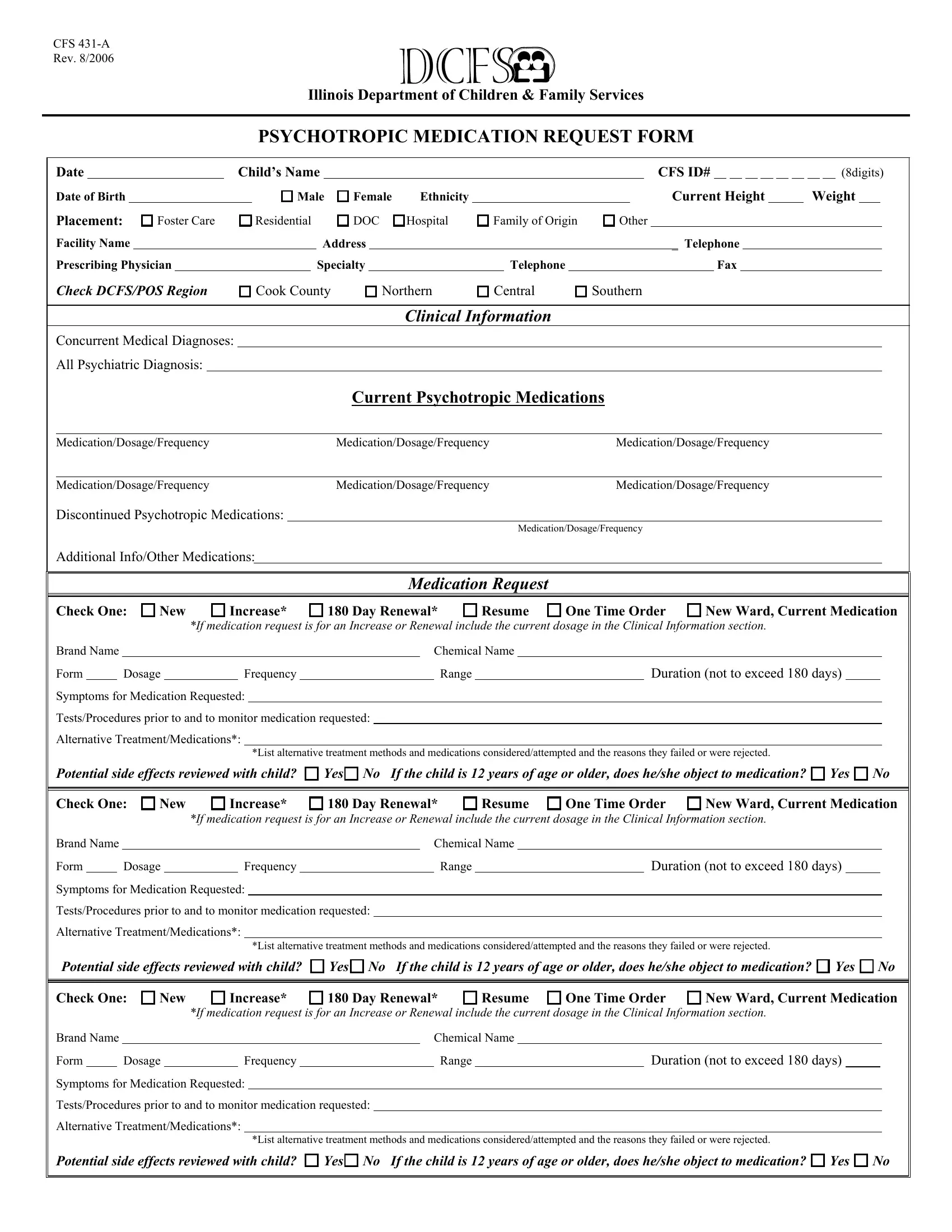
The CFS 431-A is used by Illinois DCFS to authorize psychotropic medication for children under state guardianship. The prescribing physician or psychiatrist initiates the request, the DCFS caseworker coordinates approval, and a DCFS psychotropic medication consultant reviews the clinical basis. The form supports four request types: a new medication prescription, a renewal of an existing prescription, a dosage increase, or a single-time medication order.
Who Must Complete the CFS 431-A?
The CFS 431-A must be completed jointly by the prescribing physician or psychiatrist and the assigned DCFS caseworker. The prescribing physician provides all clinical details, while the caseworker confirms the child's placement information and case status. Caregivers or foster parents may be asked to provide behavioral observations before the form is submitted.
What Information Is Required on the CFS 431-A?
Before filling out the dcfs psychotropic medication request form, gather the following:
- The child's full legal name, date of birth, and DCFS identification number
- Current placement type: foster home, relative home, residential facility, or hospital
- A complete list of current psychotropic medications with exact dosages and frequencies
- The proposed medication's brand name, chemical name, dosage form, frequency, and duration
- The request type: new prescription, renewal, dosage increase, or single-time order
- The primary diagnosis and specific target symptoms being addressed
- Documentation of non-medication interventions that were considered or attempted
- The prescribing physician's name, license number, and signature
How to Fill Out the CFS 431-A Form Online for Free
Step 1: Click "Get Form" at the top of this page to open the CFS 431-A in the FormsPal editor. No software download is required.
Step 2: Fill in the child identification section. Enter the child's name, date of birth, DCFS ID number, and current placement type.
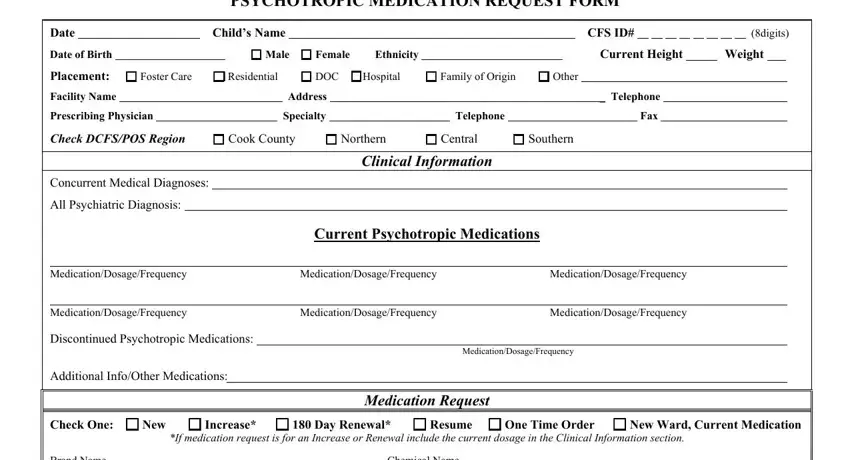
Step 3: List all current psychotropic medications. Include brand name, chemical name, dosage form, frequency, and dosage range for each currently prescribed medication.
Step 4: Complete the proposed medication section. Select the request type and enter the brand name, chemical name, dosage, frequency, dosage range, and duration for the proposed medication.
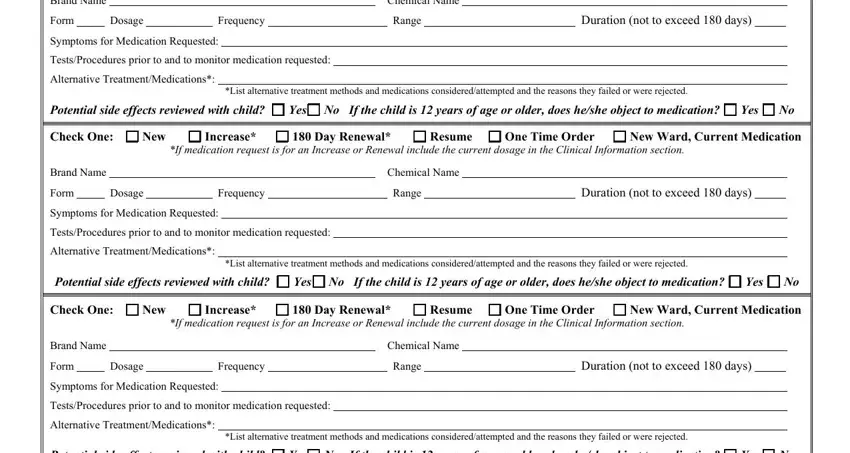
Step 5: Document the clinical justification. List the diagnosis, the target symptoms, any tests or procedures performed, and all alternative treatments considered.
Step 6: Address the informed consent section. Confirm that potential side effects were reviewed with the caregiver. For children 12 and older, document whether the child consents to or objects to the medication. This field is mandatory.
Step 7: Have the prescribing physician sign and date the form. Review all fields for accuracy before the caseworker submits the completed CFS 431-A to DCFS for approval.
What Are Common Mistakes on the CFS 431-A Form?
These errors frequently delay CFS 431-A approval or result in rejection:
- Incomplete medication lists: All current psychotropic medications must be listed, even those unrelated to the new request. Omitting an active prescription is a common cause of rejection.
- Missing alternative treatment documentation: DCFS requires proof that non-medication interventions were considered before the request. Leaving this section blank delays approval.
- Wrong request type selected: Choosing the wrong category (new vs. renewal vs. increase) causes administrative delays. Verify the correct type with the physician before submitting.
- Child consent section left blank: For children 12 and older, documenting consent or objection is mandatory. This field cannot be skipped.
- Missing physician signature: The form is invalid without the prescribing physician's dated signature. This step must be completed before submission.
What Other Illinois DCFS Forms Are Available on FormsPal?
FormsPal provides many Illinois DCFS forms for child welfare case management. These forms are commonly used alongside the CFS 431-A:
- CFS 508-1 Form - Illinois DCFS administrative form for child welfare documentation
- CFS 597-A Form - DCFS supplemental case record used with placement documentation
- CFS 602 Form - Illinois DCFS case plan document for children in care
- CFS 718-B Form - DCFS form used in residential care settings
- DCFS 561-B Form - Illinois DCFS service plan and visitation documentation