CFS 62 Child Care Enrollment Form Details
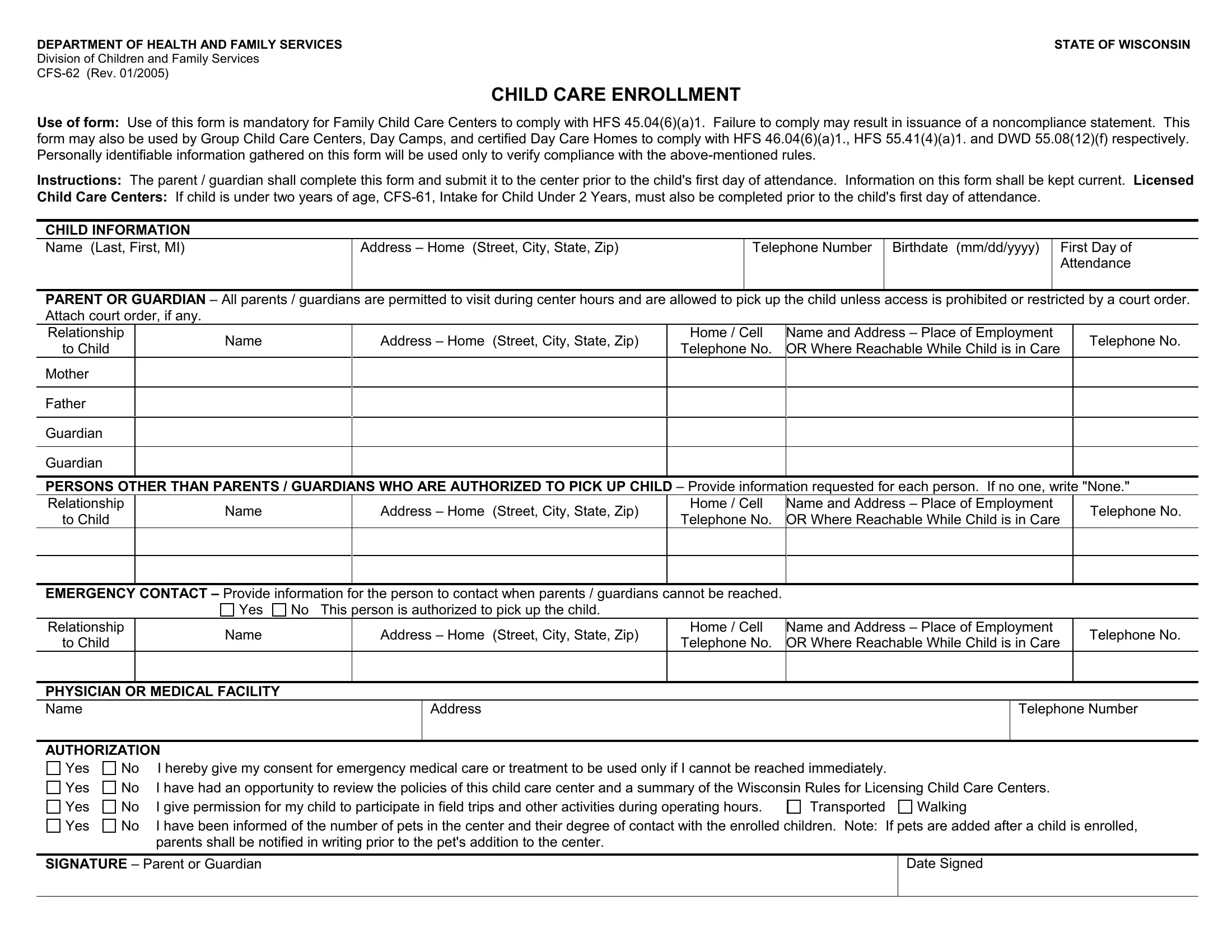
The CFS-62 form was issued by the Wisconsin Department of Health and Family Services, Division of Children and Family Services. It was last revised in January 2005. The form is required for enrolling children in family child care centers, group child care centers, day camps, and certified day care homes. State regulations (HFS 45, HFS 46, HFS 55, and DWD 55) require the completed form on file before a child's first day. It must be updated any time the child's information changes.
What Information Does the CFS 62 Form Collect?
Parents or guardians fill out the CFS-62 to give the care facility the details it needs to keep the child safe. The form captures six categories of information:
- Child's personal details - full legal name, date of birth, and home address
- Parent or guardian contact info - name, address, daytime and evening phone numbers
- Emergency contacts - at least two people who can be reached when parents are unavailable, with their relationship noted
- Authorized pickup persons - names of all adults permitted to pick up the child from the facility
- Medical information - health insurance details, known allergies, and current medical conditions
- Parental permissions - consent for medical care, field trips, swimming, and contact with animals at the facility
How to Complete the CFS 62 Child Care Enrollment Form
Follow these steps to fill out the Wisconsin CFS-62 correctly:
- Enter the child's full legal name, date of birth, and home address in the child information section.
- Provide at least one parent or guardian name, home address, and both daytime and evening phone numbers.
- List a minimum of two emergency contacts. Include their full name, phone number, and relationship to the child.
- Write down every adult who is authorized to pick up your child. Include their full name and relationship.
- Enter your child's health insurance provider name and policy number. Note any allergies or ongoing medical conditions.
- Review the permissions section. Check each box that applies for medical treatment, field trips, swimming, and animal contact.
- Sign and date the form. Return it to the care facility before your child's first day.
Frequently Asked Questions
Is the CFS 62 the same as the child care enrollment form?
Yes. The CFS-62 is Wisconsin's official child care enrollment form. Different facilities may call it the ChildCareEnrollment form or simply the child care enrollment form. It is the same document.
How long does it take to fill out the CFS-62?
Most parents finish the form in 10 to 15 minutes when all required information is ready.
What happens if the information changes?
Notify your care provider right away. Wisconsin rules require the form to be kept current. You can also find the Child Enrollment Packet and the Daycare Registration Form on FormsPal for additional paperwork your facility may require.
Does the CFS 62 form expire?
There is no formal expiration date. However, facilities must always have current information on file. Update the form whenever emergency contacts, health insurance, or medical conditions change. See also the Child Care Incident Report for recording events at the facility.
| Question | Answer |
|---|
| Form Name | CFS 62 Child Care Enrollment Form |
| Form Length | 1 page |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 min |
| Other names | child care enrollment form, ChildCareEnrollment, CFS-62 |