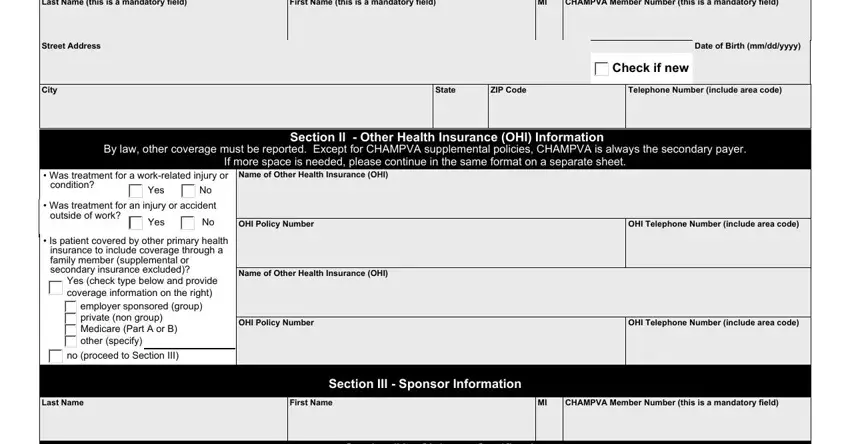
 Check if new
Check if new employer sponsored (group) private (non group)
employer sponsored (group) private (non group) Medicare (Part A or B) other (specify)
Medicare (Part A or B) other (specify)
 no (proceed to Section III)
no (proceed to Section III)
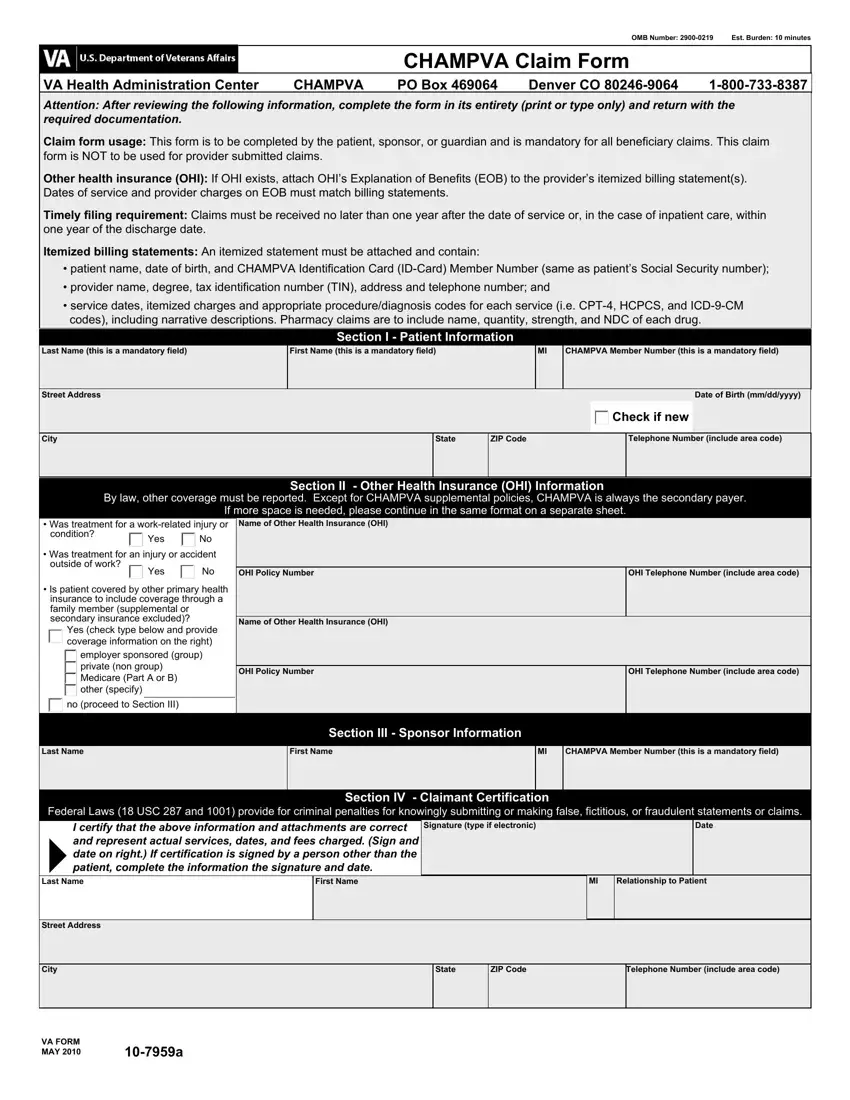
Filling in documents using our PDF editor is easier compared to nearly anything. To modify champva claim forms printable the document, there isn't anything you need to do - basically continue with the steps below:
Step 1: Click the "Get Form Now" button to get going.
Step 2: Now you are going to be on the form edit page. You'll be able to add, change, highlight, check, cross, add or delete areas or phrases.
All of these parts are included in the PDF template you'll be filling out.
Note the demanded details in the box Federal Laws USC and provide, I certify that the above, Signature type if electronic, Date, Last Name, First Name, Relationship to Patient, Street Address, City, VA FORM MAY, State, ZIP Code, and Telephone Number include area code.
Step 3: Choose the "Done" button. You can now export your PDF form to your electronic device. As well as that, you'll be able to forward it by means of electronic mail.
Step 4: Make sure you stay clear of potential issues by creating around two duplicates of the file.
