
Using PDF files online is always super easy using our PDF tool. You can fill in dhs 2240 form here painlessly. To have our editor on the forefront of convenience, we aim to put into practice user-oriented features and improvements on a regular basis. We are always looking for suggestions - assist us with remolding the way you work with PDF docs. Here is what you'd need to do to begin:
Step 1: Hit the "Get Form" button above. It'll open up our pdf editor so you could begin completing your form.
Step 2: This editor enables you to customize nearly all PDF documents in a variety of ways. Enhance it by writing any text, adjust existing content, and place in a signature - all within a couple of clicks!
This form requires specific data to be entered, hence you need to take your time to type in what is expected:
1. The dhs 2240 form will require certain details to be typed in. Be sure that the subsequent blanks are complete:
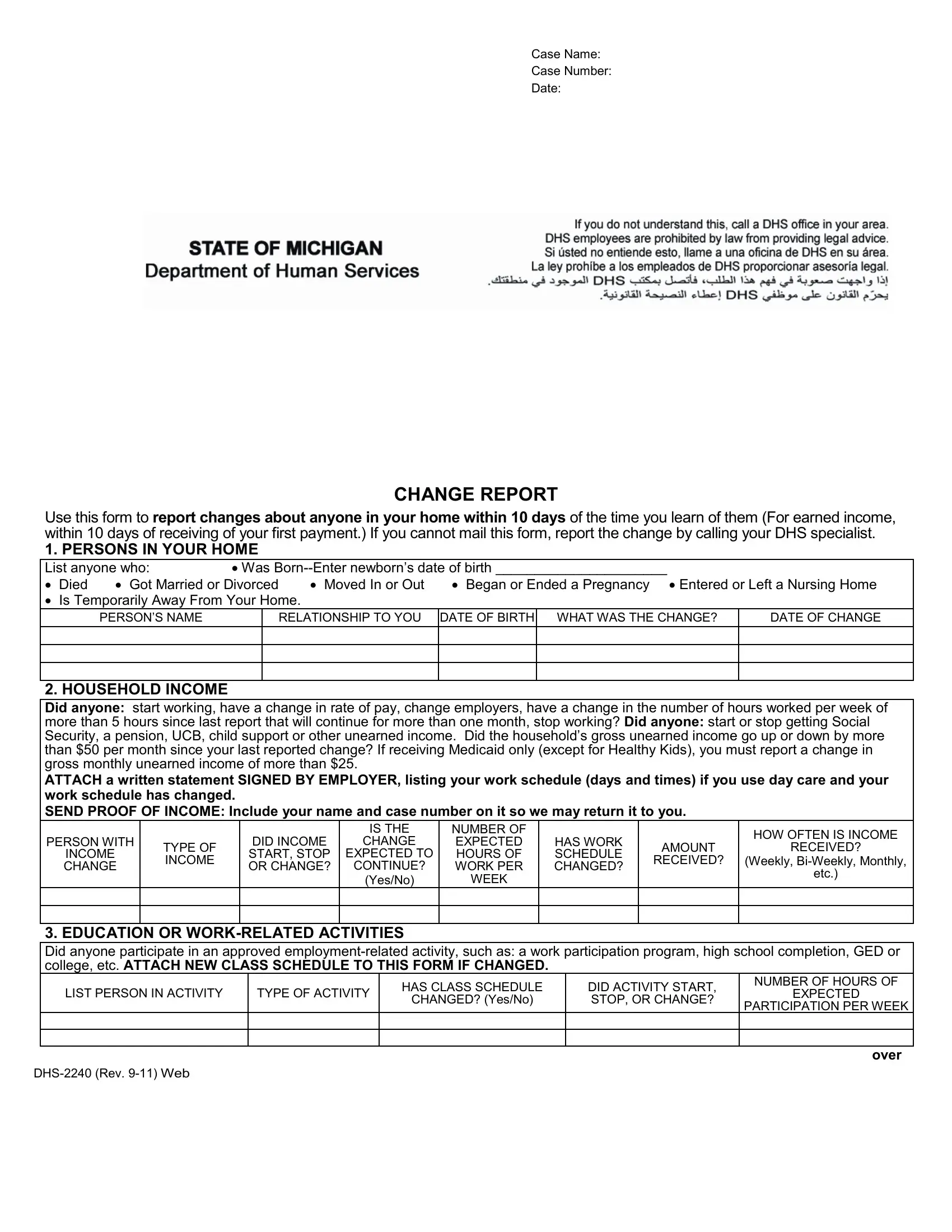
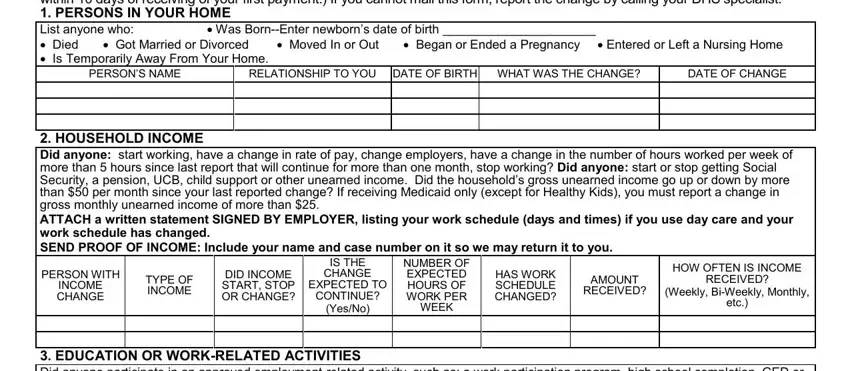
2. Once your current task is complete, take the next step – fill out all of these fields - Use this form to report changes, PERSONS NAME, RELATIONSHIP TO YOU DATE OF BIRTH, DATE OF CHANGE, HOUSEHOLD INCOME Did anyone start, PERSON WITH, INCOME CHANGE, TYPE OF INCOME, DID INCOME START STOP OR CHANGE, IS THE CHANGE, EXPECTED TO CONTINUE, YesNo, NUMBER OF EXPECTED HOURS OF WORK, WEEK, and HAS WORK SCHEDULE CHANGED with their corresponding information. Make sure to double check that everything has been entered correctly before continuing!
3. In this particular stage, have a look at EDUCATION OR WORKRELATED, NUMBER OF HOURS OF, LIST PERSON IN ACTIVITY, TYPE OF ACTIVITY, EXPECTED, DID ACTIVITY START STOP OR CHANGE, CHANGED YesNo, PARTICIPATION PER WEEK, DHS Rev Web, and over. These have to be filled in with utmost precision.
4. Now fill out this fourth part! In this case you will have all these CHILD DAY CARE OR DISABLED ADULT, REASON FOR CAREWork, PROVIDER ID, DATE OF CHANGE, NAME OF THE PROVIDER, AGE, NUMBER, School Training MedicalSocial, CARE, a b c d PERSON RECEIVING CARE List, person as above, DAYS AND TIMES CARE IS, PROVIDED, IS CARE PROVIDED IN CHILDS, and HOME fields to do.
It's easy to make errors while filling in your DATE OF CHANGE, and so be sure to reread it prior to deciding to send it in.
5. As a final point, the following final segment is precisely what you have to finish prior to finalizing the PDF. The blanks in this instance are the following: Do you expect the changes you, Yes, I understand that the information, I CERTIFY THAT THE STATEMENTS ON, Clients Signature or Mark, Date, Clients Telephone Number, Date, Signature of Other Person, Department of Human Services DHS, PENALTY Loss of eligibility for, COMPLETION Voluntary, and DHS Rev Web.
Step 3: Once you've reread the information you given, simply click "Done" to finalize your form at FormsPal. Join us now and easily gain access to dhs 2240 form, prepared for download. Every single edit you make is handily saved , so that you can change the document at a later time anytime. Whenever you work with FormsPal, you'll be able to complete forms without worrying about personal data incidents or entries getting distributed. Our protected software helps to ensure that your personal data is maintained safely.