
Handling PDF files online is always very easy using our PDF editor. You can fill out ldss 4310 periodic report here within minutes. The tool is constantly upgraded by our staff, getting additional functions and turning out to be better. With some simple steps, you'll be able to start your PDF editing:
Step 1: Hit the orange "Get Form" button above. It will open our pdf editor so that you could start filling out your form.
Step 2: The editor will let you change PDF documents in a range of ways. Transform it by writing customized text, correct existing content, and include a signature - all readily available!
Completing this form requires thoroughness. Ensure every field is filled in correctly.
1. Whenever filling out the ldss 4310 periodic report, make certain to include all essential blank fields within its corresponding form section. This will help to facilitate the work, enabling your details to be handled quickly and correctly.
2. Once the previous section is completed, you're ready include the required details in You must answer all questions on, You must complete and sign this, or your Child Assistance CAP Child, and Reminder If you are also receiving in order to proceed to the 3rd stage.
Always be extremely mindful while filling out or your Child Assistance CAP Child and You must answer all questions on, as this is where a lot of people make some mistakes.
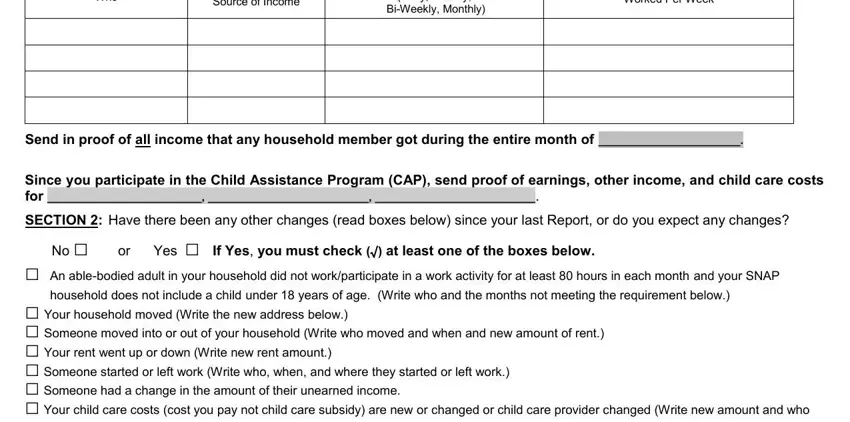
3. This part will be hassle-free - fill out every one of the fields in Who, Source of Income, Daily Weekly, BiWeekly Monthly, Worked Per Week, Send in proof of all income that, Since you participate in the Child, SECTION Have there been any other, household does not include a child, and No or Yes If Yes you must check to conclude this process.
4. The fourth subsection comes next with the following form blanks to focus on: No or Yes If Yes you must check, provides the child care, Write the details of your changes, CERTIFICATION I understand that, I understand that I must contact, I understand that I must contact, For my SNAP case I must report, Your Signature, Fill Out Return In The Envelope, When you return this Report make, and Telephone Number daytime.
Step 3: Before finalizing your form, you should make sure that blanks are filled out the right way. Once you are satisfied with it, click on “Done." Try a free trial account with us and obtain instant access to ldss 4310 periodic report - which you can then make use of as you want in your personal cabinet. FormsPal offers protected document completion devoid of personal data recording or distributing. Be assured that your information is in good hands with us!