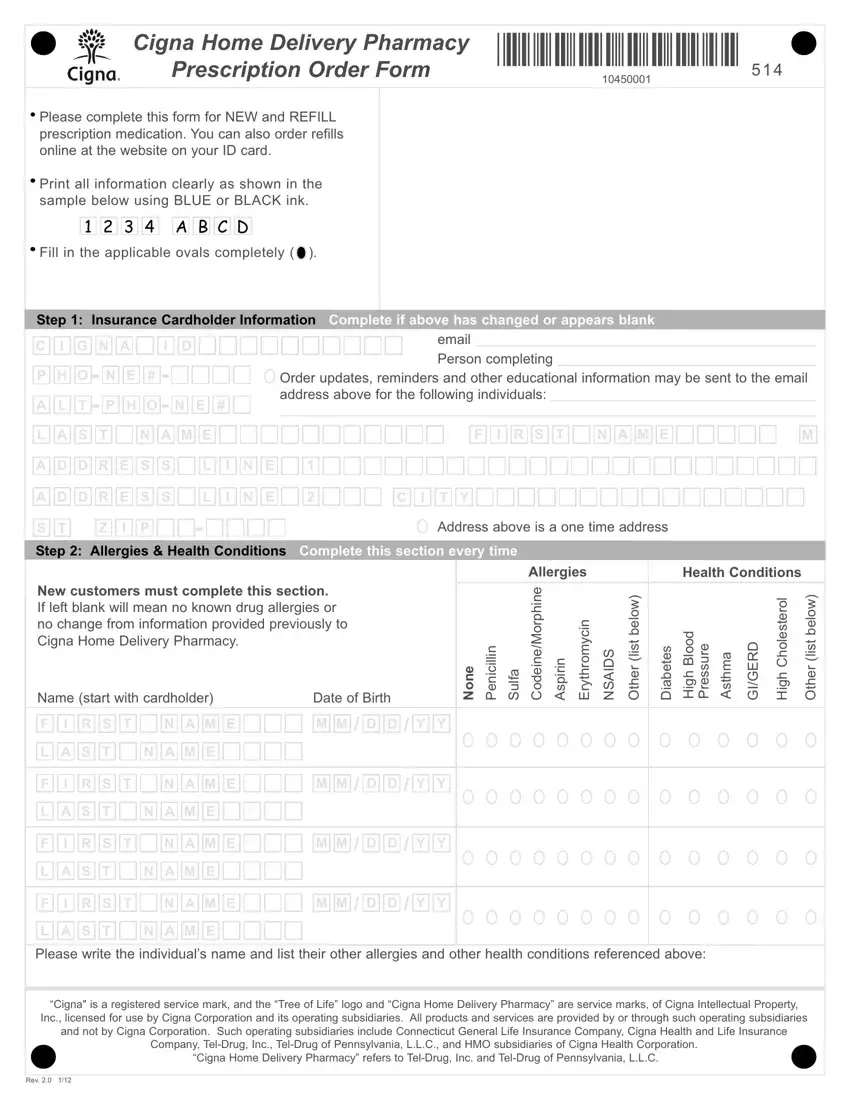
 Please complete this form for NEW and REFILL prescription medication. You can also order refills online at the website on your ID card.
Please complete this form for NEW and REFILL prescription medication. You can also order refills online at the website on your ID card. Print all information clearly as shown in the sample below using BLUE or BLACK ink.
Print all information clearly as shown in the sample below using BLUE or BLACK ink.
 2
2
 3
3
 4
4
 A
A
 B
B
 C
C
 D
D Fill in the applicable ovals completely (
Fill in the applicable ovals completely ( )
)

















 /
/



 ) “Brand Only”, you may be responsible for a higher cost.
) “Brand Only”, you may be responsible for a higher cost.We chose the best web programmers to set-up the PDF editor. The software will permit you to fill out the cigna home delivery form file with no trouble and won't require a lot of your time. This straightforward guideline will enable you to begin.
Step 1: The initial step would be to choose the orange "Get Form Now" button.
Step 2: Now, you can edit the cigna home delivery form. This multifunctional toolbar makes it easy to include, remove, transform, highlight, as well as do several other commands to the words and phrases and fields within the file.
Provide the content requested by the platform to fill in the file.
You need to submit the Name start with cardholder, Date of Birth, c n e P, e n o N, u S, e n h p r o M e n e d o C, t y r E, S D A S N, n i r i p s A, r e h O, e b a D, t s e o h C h g H, r e h O, e r u s s e r P, and a m h t s A box with the demanded particulars.
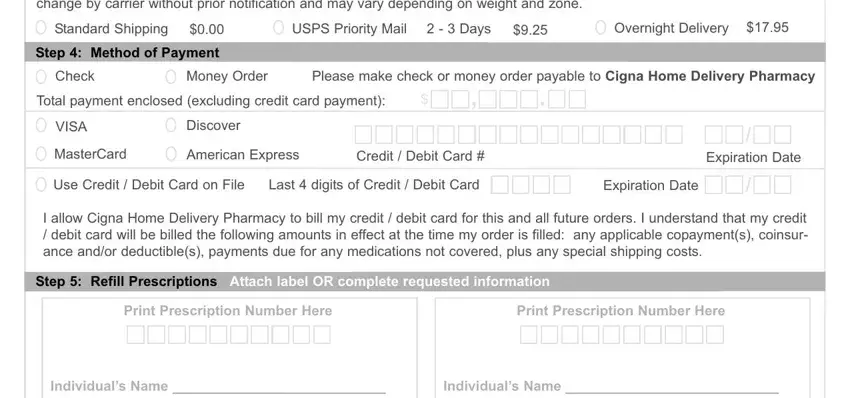
You need to point out the essential particulars in the Refrigerated shipments will be, Standard Shipping, USPS Priority Mail, Days, Overnight Delivery, Step Method of Payment, Check, Money Order, Please make check or money order, Total payment enclosed excluding, VISA, Discover, MasterCard, American Express, and Credit Debit Card field.
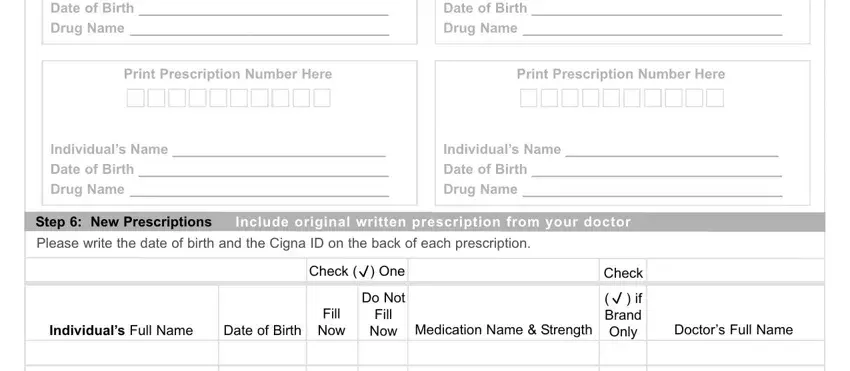
The Individuals Name Date of Birth, Individuals Name Date of Birth, Print Prescription Number Here, Print Prescription Number Here, Individuals Name Date of Birth, Individuals Name Date of Birth, Step New Prescriptions, Include original written, Please write the date of birth and, Individuals Full Name, Date of Birth, Check One, Do Not Fill Now Medication Name, Fill Now, and Check space is where both parties can put their rights and obligations.
Finalize by checking the next sections and filling in the proper information: Pharmacy law allows pharmacists to, and Remember to include the original.
Step 3: As you select the Done button, your finalized document can be simply transferred to any kind of your gadgets or to electronic mail indicated by you.
Step 4: Generate copies of your file - it will help you avoid upcoming concerns. And don't get worried - we don't display or read your data.
