
Using PDF forms online is always super easy using our PDF editor. You can fill out small claims court nyc forms here and use many other functions we provide. In order to make our tool better and easier to use, we consistently implement new features, taking into account feedback coming from our users. To get the process started, consider these easy steps:
Step 1: Click the orange "Get Form" button above. It's going to open up our tool so you can begin completing your form.
Step 2: With the help of this handy PDF editing tool, you may do more than merely complete blank form fields. Edit away and make your docs seem great with custom text incorporated, or modify the file's original input to excellence - all that comes with an ability to add stunning photos and sign the PDF off.
To be able to complete this document, be certain to provide the right information in each area:
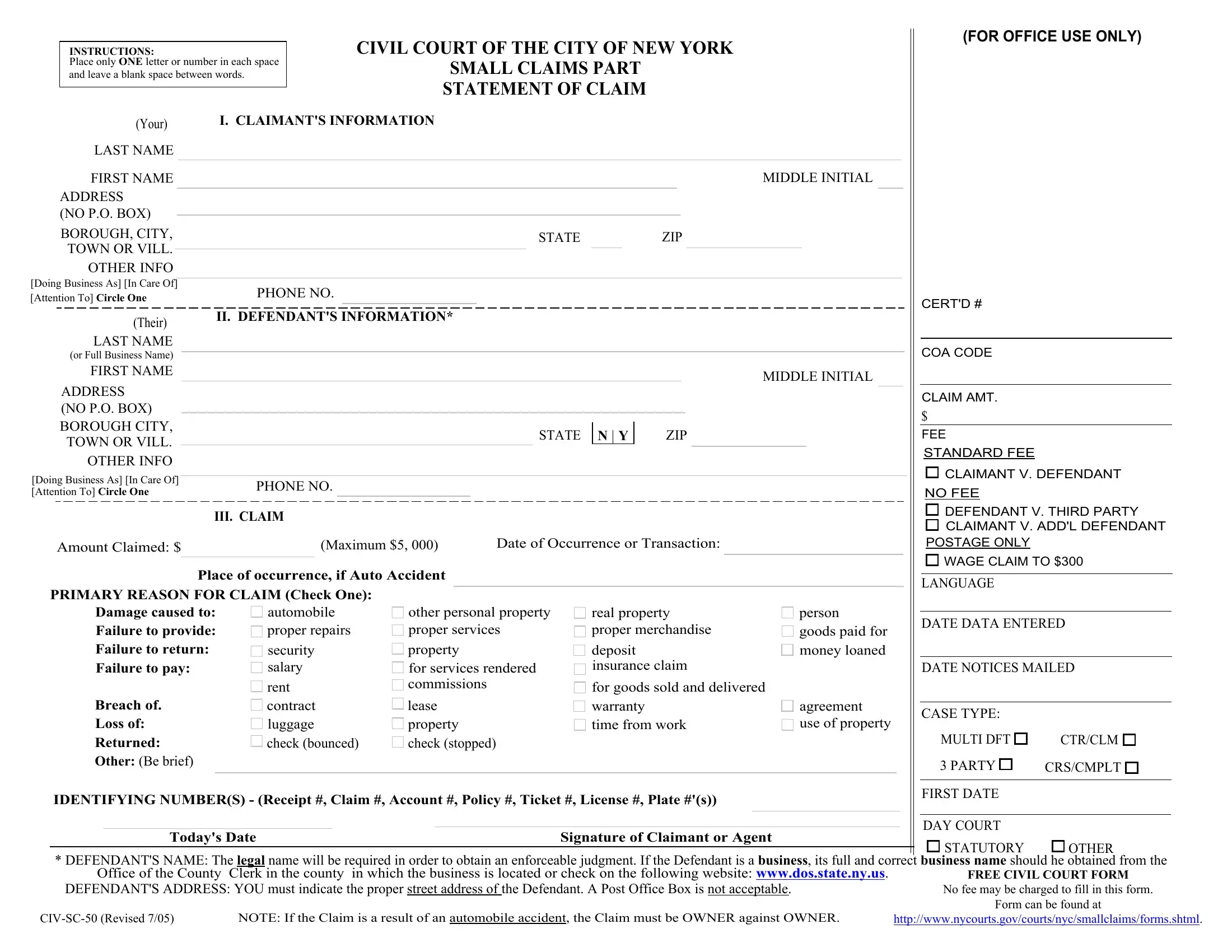
1. Begin completing the small claims court nyc forms with a group of essential blank fields. Gather all the necessary information and ensure not a single thing missed!
2. After the last array of blank fields is filled out, proceed to type in the suitable information in these - Damage caused to Failure to, Breach of Loss of, Returned Other Be brief, security salary, rent contract luggage check bounced, property for services rendered, lease property check stopped, deposit insurance claim, for goods sold and delivered, IDENTIFYING NUMBERS Receipt, Todays Date, Signature of Claimant or Agent, DATE NOTICES MAILED, person goods paid for money loaned, and agreement use of property.
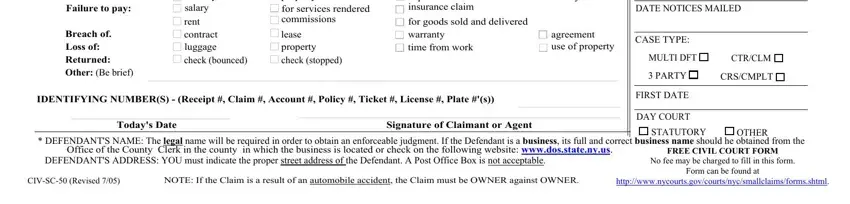
Those who use this document often get some points incorrect while filling out Returned Other Be brief in this area. You should definitely review whatever you type in here.
Step 3: Confirm that your details are accurate and click on "Done" to complete the project. Join us now and immediately get access to small claims court nyc forms, ready for download. All alterations made by you are kept , letting you customize the form at a later stage when necessary. FormsPal provides secure form editor devoid of data record-keeping or sharing. Rest assured that your information is safe with us!