


You can prepare hhs civil rights request effectively with the help of our online editor for PDFs. The editor is constantly maintained by our staff, acquiring useful features and turning out to be much more convenient. This is what you'd have to do to begin:
Step 1: Hit the "Get Form" button in the top part of this page to access our PDF tool.
Step 2: Using this handy PDF tool, it is possible to accomplish more than simply fill out blank fields. Express yourself and make your forms seem sublime with customized text incorporated, or tweak the file's original content to perfection - all that comes along with the capability to add any images and sign the PDF off.
This document will involve some specific details; in order to ensure accuracy and reliability, please pay attention to the suggestions hereunder:
1. The hhs civil rights request involves certain details to be entered. Ensure that the following blanks are filled out:
2. The subsequent step is usually to fill out these particular blank fields: Go to.
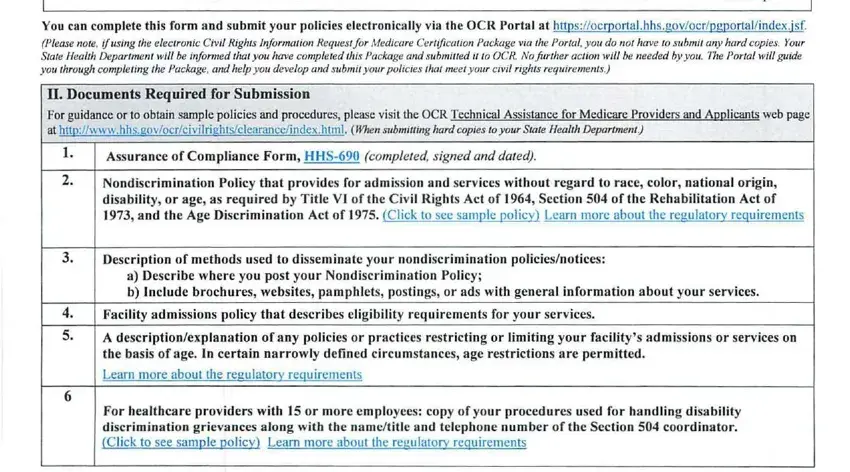
3. Completing httpwwwhhsgovocrlep This guidance, Technical Assistance for Medicare, Examples of Vital Written Materials, Vital written materials could, Consent and complaint forms, Intake forms with the potential, Written notices of eligibility, actions affecting parental custody, Notices advising LEP persons of, Written tests that do not assess, and particular license job or skill is essential for the next step, make sure to fill them out in their entirety. Don't miss any details!
4. You're ready to proceed to the next part! Here you'll get all of these Resources, US Department of Justice at, and ADA Business Brief Communicating form blanks to complete.
5. When you draw near to the conclusion of this file, there are actually a couple extra points to undertake. Particularly, A new online library of ADA should all be filled in.
As for A new online library of ADA and A new online library of ADA, make sure you get them right here. These two are considered the key ones in the file.
Step 3: Go through all the details you've typed into the form fields and then press the "Done" button. Find your hhs civil rights request after you register online for a free trial. Immediately get access to the form from your FormsPal cabinet, along with any edits and changes conveniently synced! FormsPal offers safe document editor with no personal data recording or any kind of sharing. Be assured that your data is secure with us!