
 AAHHS/HFAP
AAHHS/HFAP

 01 Religious Affiliation
01 Religious Affiliation
 02 Private Nonprofit
02 Private Nonprofit
 03 Other Nonprofit
03 Other Nonprofit
 04 Proprietary
04 Proprietary
 05 City
05 City
 06 County
06 County
 07 State
07 State
 08 Federal
08 Federal
 09 Other Government
09 Other Government Yes
Yes  No
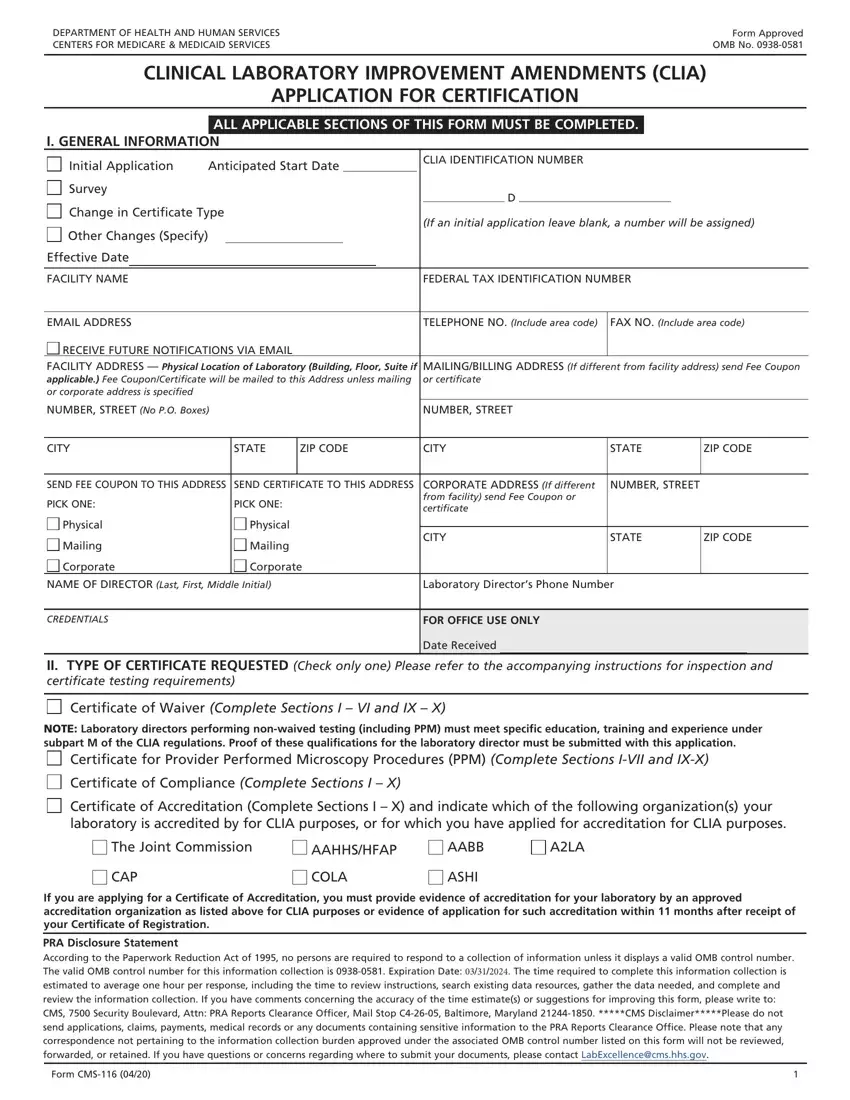
NoCompleting the clia waiver file is not hard using our PDF editor. Follow the following steps to prepare the document right away.
Step 1: On this web page, select the orange "Get form now" button.
Step 2: Now you are equipped to enhance clia waiver. You have a wide range of options thanks to our multifunctional toolbar - you'll be able to add, erase, or customize the content material, highlight its certain parts, and undertake other sorts of commands.
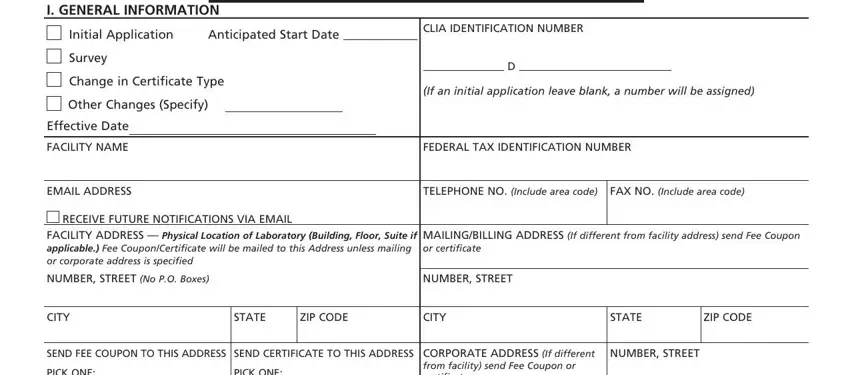
To be able to fill in the clia waiver PDF, enter the information for each of the sections:
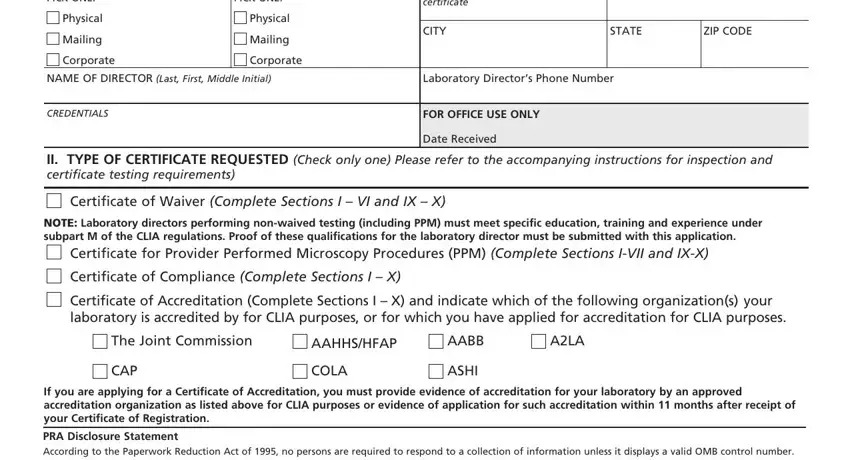
Within the part PICK ONE, PICK ONE, CORPORATE ADDRESS If different, Physical, Mailing, Corporate, Physical, Mailing, Corporate, CITY, STATE, ZIP CODE, NAME OF DIRECTOR Last First Middle, Laboratory Directors Phone Number, and CREDENTIALS write down the details the application demands you to do.
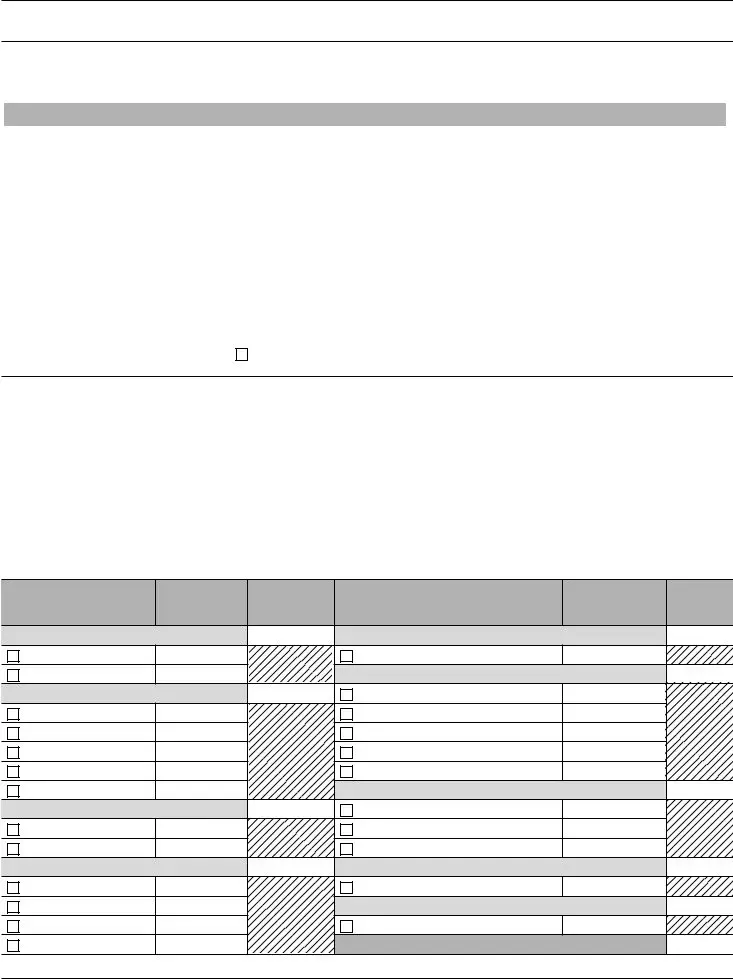
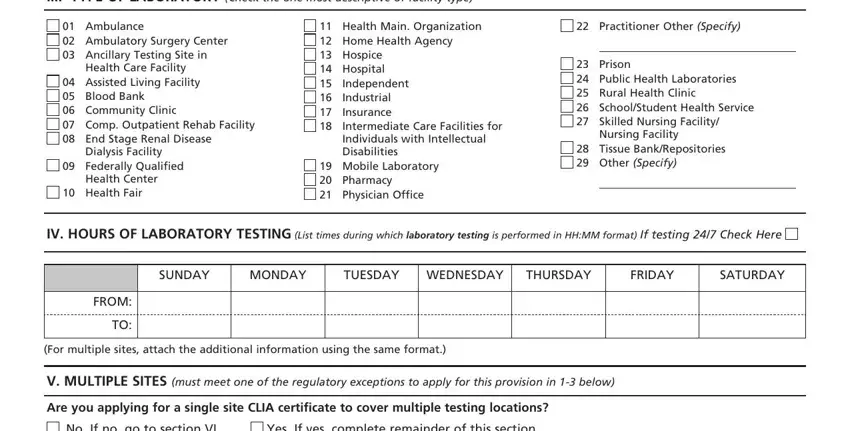
It's important to provide particular data within the box III TYPE OF LABORATORY Check the, Ambulance Ambulatory Surgery, Dialysis Facility Federally, Health Fair, Health Main Organization Home, Independent Industrial Insurance, Practitioner Other Specify, Prison Public Health, Nursing Facility, Tissue BankRepositories Other, IV HOURS OF LABORATORY TESTING, SUNDAY, MONDAY, TUESDAY, and WEDNESDAY.
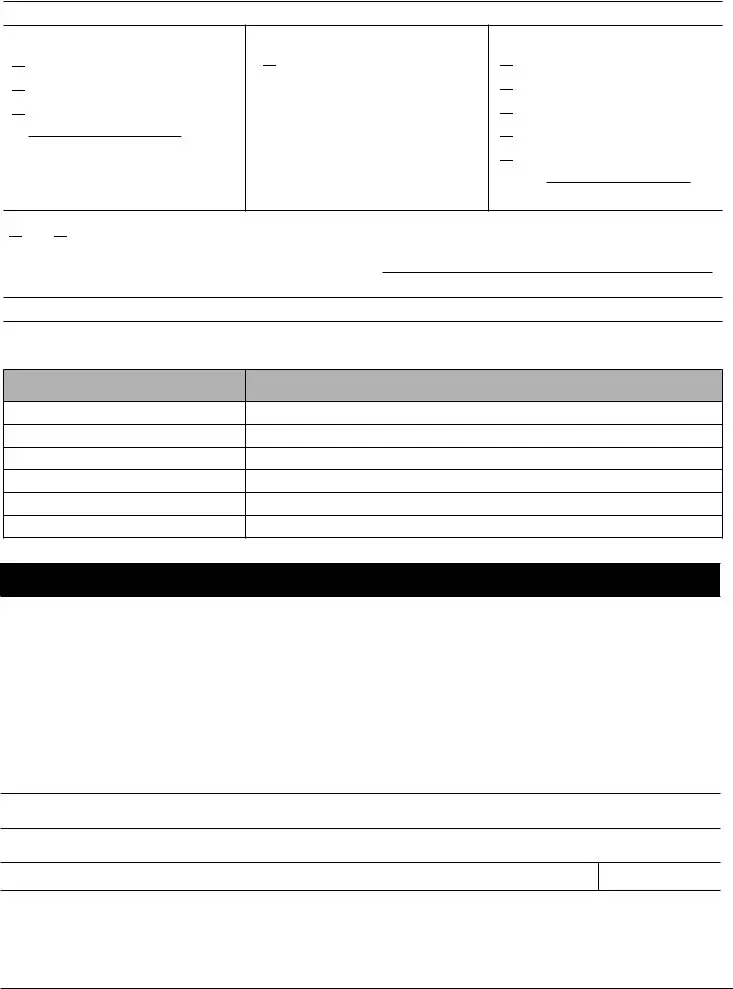
The Is this a laboratory that is not, Yes, If yes and a mobile unit is, Is this a notforprofit or Federal, Yes, If yes provide the number of sites, and list name address and test, Is this a hospital with several, Yes, If yes provide the number of sites, and list name or department, If additional space is needed, and attach the additional, NAME AND ADDRESSLOCATION, and TESTS space is the place where both parties can describe their rights and obligations.
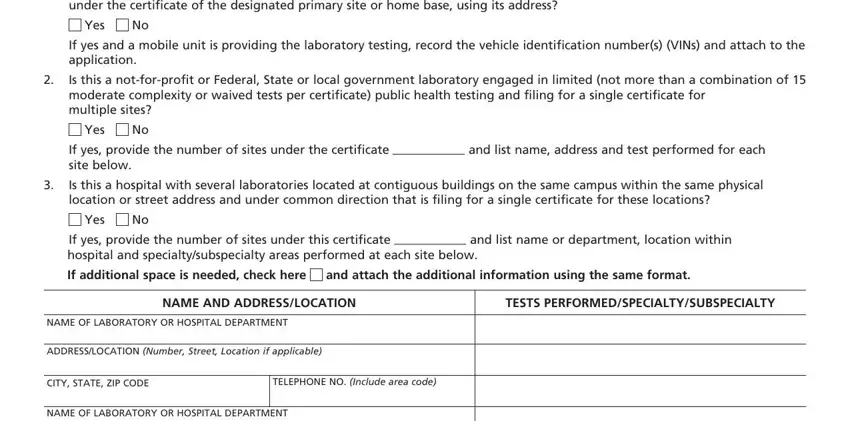
Look at the sections ADDRESSLOCATION Number Street, CITY STATE ZIP CODE, TELEPHONE NO Include area code, and Form CMS and next fill them out.

Step 3: Hit the "Done" button. Then, you may transfer the PDF document - download it to your electronic device or deliver it through email.
Step 4: Get no less than a couple of copies of the form to remain away from any specific future concerns.
