

In case you would like to fill out medicare form cms 460, you don't need to download any kind of applications - just use our PDF tool. To retain our editor on the cutting edge of practicality, we work to implement user-oriented capabilities and enhancements on a regular basis. We are always grateful for any feedback - join us in reshaping how you work with PDF forms. To get the ball rolling, consider these easy steps:
Step 1: First of all, open the editor by clicking the "Get Form Button" above on this webpage.
Step 2: Using our handy PDF file editor, you can accomplish more than merely fill out blanks. Edit away and make your docs appear perfect with customized text incorporated, or modify the file's original content to excellence - all accompanied by the capability to insert almost any images and sign it off.
With regards to the fields of this particular PDF, here is what you need to do:
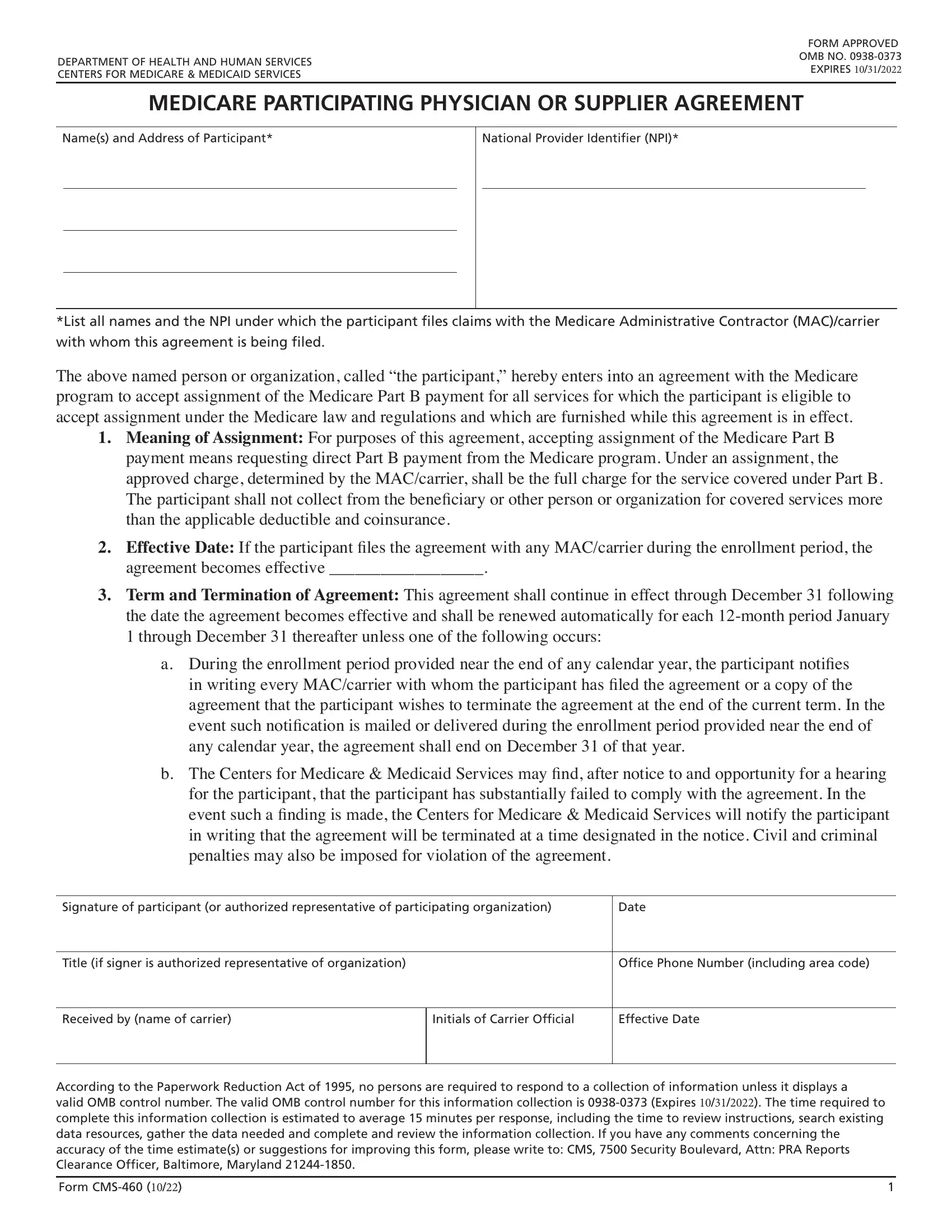
1. Fill out your medicare form cms 460 with a group of major blanks. Consider all the information you need and be sure nothing is missed!
2. Once your current task is complete, take the next step – fill out all of these fields - Signature of participant or, Date, Title if signer is authorized, Office Phone Number including area, Received by name of carrier, Initials of Carrier Official, Effective Date, and According to the Paperwork with their corresponding information. Make sure to double check that everything has been entered correctly before continuing!
Always be extremely careful while filling out Date and According to the Paperwork, since this is the part in which most users make errors.
Step 3: Ensure that your details are right and then press "Done" to proceed further. Get hold of your medicare form cms 460 once you sign up at FormsPal for a 7-day free trial. Immediately access the pdf form from your FormsPal account, along with any edits and changes conveniently preserved! FormsPal is devoted to the confidentiality of our users; we make certain that all information handled by our tool remains protected.