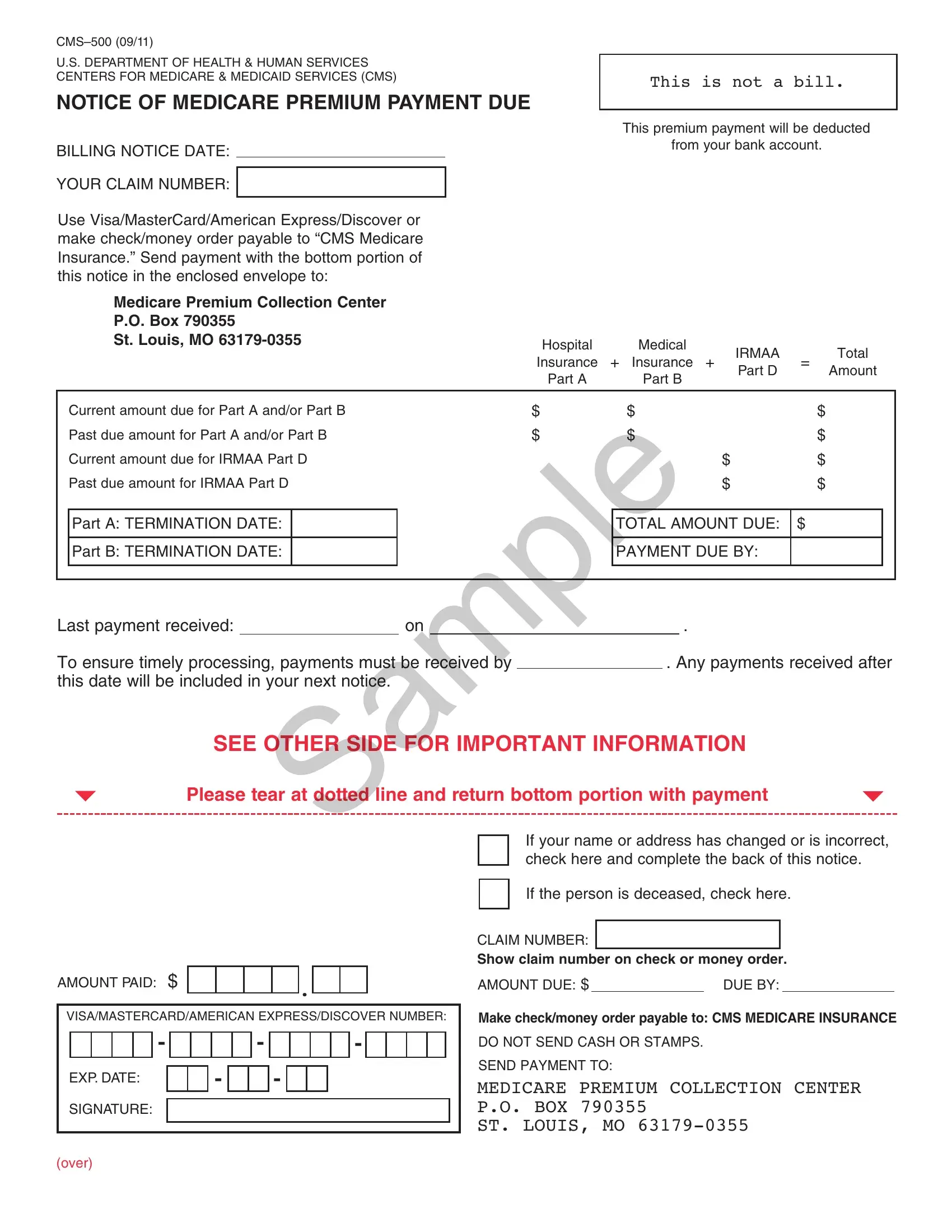
Understanding the CMS-500 form is essential for everyone who participates in the Medicare program. Issued by the U.S. Department of Health & Human Services Centers for Medicare & Medicaid Services (CMS), this document acts as a notice for Medicare premium payments due. It offers a clear breakdown of payments needed for Medicare Part A (Hospital Insurance), Part B (Medical Insurance), and the Income-Related Monthly Adjustment Amount (IRMAA) for both Part B and Part D. It's crucial not to mistake this for a bill but rather a notification specifying the total amount due for Medicare coverage, including both current and past due amounts. The form allows for payment via various methods and highlights the importance of timely payments to avoid service interruption. It comes equipped with instructions for those whose personal details have changed or for the estate of a deceased member. Its bottom section is designed for detachment and accompanying payment, providing a straightforward way to ensure Medicare coverage continues without a hitch. Moreover, the CMS-500 form includes vital customer service information for individuals with questions regarding their Medicare insurance or the payment amounts. It warns of the consequences of non-payment, such as termination of Medicare insurance and the implications for future coverage and costs. Significantly, it guides individuals toward setting up Medicare Easy Pay to automate premium payments, ensuring they're timely and reducing the risk of coverage lapses due to missed payments.
| Question | Answer |
|---|---|
| Form Name | Cms 500 Form |
| Form Length | 2 pages |
| Fillable? | Yes |
| Fillable fields | 31 |
| Avg. time to fill out | 6 min 42 sec |
| Other names | cms 500 form no download needed, cms, cms 500 premium bill, where can in get a cms 500 form for medicare |
U.S. DEPARTMENT OF HEALTH & HUMAN SERVICES
CENTERS FOR MEDICARE & MEDICAID SERVICES (CMS)
NOTICE OF MEDICARE PREMIUM PAYMENT DUE
BILLING NOTICE DATE:
YOUR CLAIM NUMBER:
Use Visa/MasterCard/American Express/Discover or make check/money order payable to “CMS Medicare Insurance.” Send payment with the bottom portion of this notice in the enclosed envelope to:
THIS IS NOT A BILL.
This premium payment will be deducted
from your bank account.
|
Medicare Premium Collection Center |
|
|
|
|
|
|
|
|
|
|
P.O. Box 790355 |
|
|
|
|
|
|
|
|
|
|
St. Louis, MO |
Hospital |
|
|
Medical |
IRMAA |
|
Total |
||
|
|
|
|
|
|
|||||
|
|
|
Insurance |
+ |
Insurance + |
= |
||||
|
|
|
Part D |
Amount |
||||||
|
|
|
Part A |
|
|
Part B |
|
|||
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
Current amount due for Part A and/or Part B |
$ |
|
|
$ |
|
|
$ |
|
|
|
Past due amount for Part A and/or Part B |
$ |
|
|
$ |
|
|
$ |
|
|
|
Current amount due for IRMAA Part D |
|
|
|
|
$ |
|
$ |
|
|
|
Past due amount for IRMAA Part D |
|
|
|
|
$ |
|
$ |
|
|
|
|
|
|
|
|
|
|
|
||
|
Part A: TERMINATION DATE: |
|
|
|
TOTAL AMOUNT DUE: |
$ |
|
|
||
|
|
|
|
|
|
|
|
|
||
|
Part B: TERMINATION DATE: |
|
|
|
PAYMENT DUE BY: |
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Last payment received: |
on |
|
|
. |
To ensure timely processing, payments must be received by |
. Any payments received after |
|||
this date will be included in your next notice. |
|
|
|
|
SEE OTHER SIDE FOR IMPORTANT INFORMATION
Please tear at dotted line and return bottom portion with payment
AMOUNT PAID: $ |
. |
|
VISA/MASTERCARD/AMERICAN EXPRESS/DISCOVER NUMBER:
|
|
|
|
- |
|
|
|
|
|
|
|
|
- |
|
|
|
|
|
|
- |
|
|
|
|
|
|
EXP. DATE: |
|
|
|
|
|
|
|
|
|
- |
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
- |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
SIGNATURE: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
If your name or address has changed or is incorrect, check here and complete the back of this notice.
If the person is deceased, check here.
CLAIM NUMBER:
Show claim number on check or money order.
AMOUNT DUE: $ |
DUE BY: |
Make check/money order payable to: CMS MEDICARE INSURANCE
DO NOT SEND CASH OR STAMPS.
SEND PAYMENT TO:
MEDICARE PREMIUM COLLECTION CENTER P.O. BOX 790355
ST. LOUIS, MO
(over)
IMPORTANT MEDICARE CUSTOMER INFORMATION
イ! If you do not pay your Part A or Part B premium, your Medicare insurance will be terminated. Even if your Medicare insurance ends, you must still pay the total premium amount you owe. You can reapply for Medicare only during the General Enrollment Period from January – March each year. If you reapply, your coverage will start on July 1 of the year you reapply, and your payment amount may be higher because your coverage was interrupted.
イ! This bill may include an Income Related Monthly Adjustment Amount (IRMAA) for Part B based on your income.
イ! If you have questions about this notice, your Medicare Part A or Part B insurance, or the amount you have to pay, please write or visit any Social Security office, or call
イ! This bill may include an IRMAA for Part D based on your income. If you do not pay the IRMAA for Part D, you will be disenrolled from your Part D prescription drug plan, even if it is part of your employer coverage or Medicare Advantage plan. If your coverage is terminated and you
イ! The IRMAA you pay for Part D may be higher than it was before because of new income or enrollment information we received from Social Security or other agencies. If you have questions about your IRMAA Part D bill amount, please call
SPECIAL MESSAGES
ABOUT THIS BILLSample
This bill shows the current amount you owe. The dates in the “Current Amount Du ” line show the months that this bill normally covers. If this is the irst bill you have received, it may a so inc ude pr miums owed for previous months not already billed. Please send your payment promptly.
MEDICARE EASY PAY
Sign up to have your Medicare premiums automatically deducted from a bank account each month and you will not have to worry about late or lost payments.
To sign up for Automated Clearing House (ACH), automated premium payment deductions from your checking or savings account, call
PAYMENTS BY CHECK
When you pay by check, you authorize the Medicare Pre ium Collection Center (MPCC) to use the information from your check to make a
as the same day your payment is received. You will not get your check back from your bank. If the MPCC cannot process your payment electronically, it will be processed as check transaction. Your bank statement will show the transaction as “CMS Medicare” and this is your proof of payment.
IF YOUR NAME OR ADDRESS HAS CHANGED OR IS DIFFERENT FROM THE NAME OR ADDRESS SHOWN ON THE FRONT OF THE FORM, PLEASE PRINT CORRECT INFORMATION BELOW:
Last Name:
Street
Number:
P.O.
Box:
City:
First
Name:
Street
Name:
Apartment
Number:
State: |
|
|
Zip |
|
|
Code: |
|
|
|
|
MI:
–