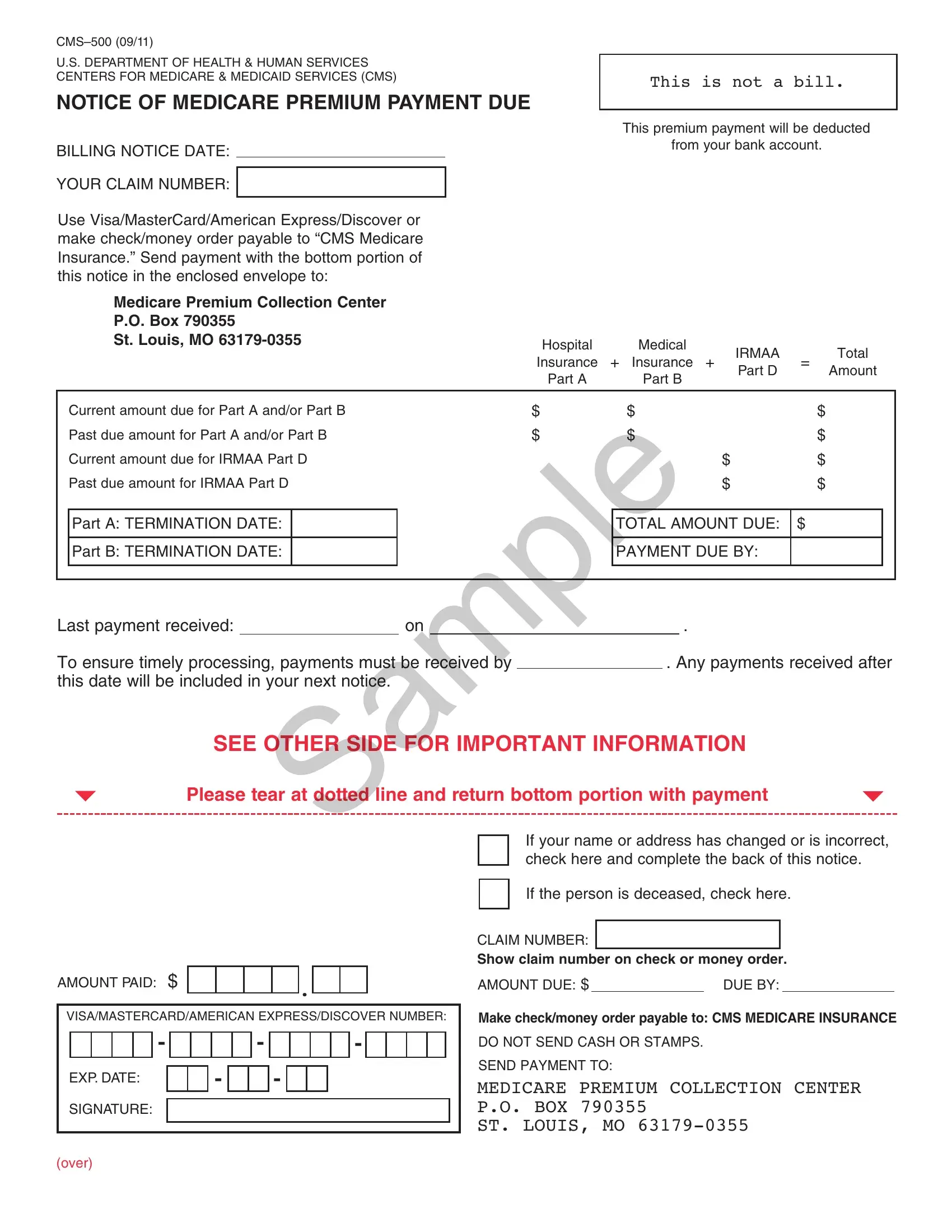
Understanding the CMS-500 form is essential for everyone who participates in the Medicare program. Issued by the U.S. Department of Health & Human Services Centers for Medicare & Medicaid Services (CMS), this document acts as a notice for Medicare premium payments due. It offers a clear breakdown of payments needed for Medicare Part A (Hospital Insurance), Part B (Medical Insurance), and the Income-Related Monthly Adjustment Amount (IRMAA) for both Part B and Part D. It's crucial not to mistake this for a bill but rather a notification specifying the total amount due for Medicare coverage, including both current and past due amounts. The form allows for payment via various methods and highlights the importance of timely payments to avoid service interruption. It comes equipped with instructions for those whose personal details have changed or for the estate of a deceased member. Its bottom section is designed for detachment and accompanying payment, providing a straightforward way to ensure Medicare coverage continues without a hitch. Moreover, the CMS-500 form includes vital customer service information for individuals with questions regarding their Medicare insurance or the payment amounts. It warns of the consequences of non-payment, such as termination of Medicare insurance and the implications for future coverage and costs. Significantly, it guides individuals toward setting up Medicare Easy Pay to automate premium payments, ensuring they're timely and reducing the risk of coverage lapses due to missed payments.
| Question | Answer |
|---|---|
| Form Name | CMS-500 Form |
| Issued by | Centers for Medicare and Medicaid Services (CMS) |
| Purpose | Medicare premium payment notice |
| Parts covered | Medicare Part A, Part B, and Part D |
| Form Length | 2 pages |
| Fillable? | Yes |
| Fillable fields | 31 |
| Avg. time to fill out | 6 min 42 sec |
| Other names | cms 500 form no download needed, cms 500 premium bill, medicare premium bill, where can I get a cms 500 form for medicare |