
form cms 700 can be filled out very easily. Just use FormsPal PDF tool to complete the task right away. FormsPal team is committed to providing you the perfect experience with our tool by continuously introducing new capabilities and improvements. With all of these updates, using our tool gets better than ever! For anyone who is seeking to get started, this is what it will take:
Step 1: First, open the tool by pressing the "Get Form Button" at the top of this webpage.
Step 2: The tool lets you work with your PDF in a variety of ways. Modify it by including any text, adjust existing content, and place in a signature - all when it's needed!
This form needs some specific details; in order to ensure accuracy, remember to adhere to the following recommendations:
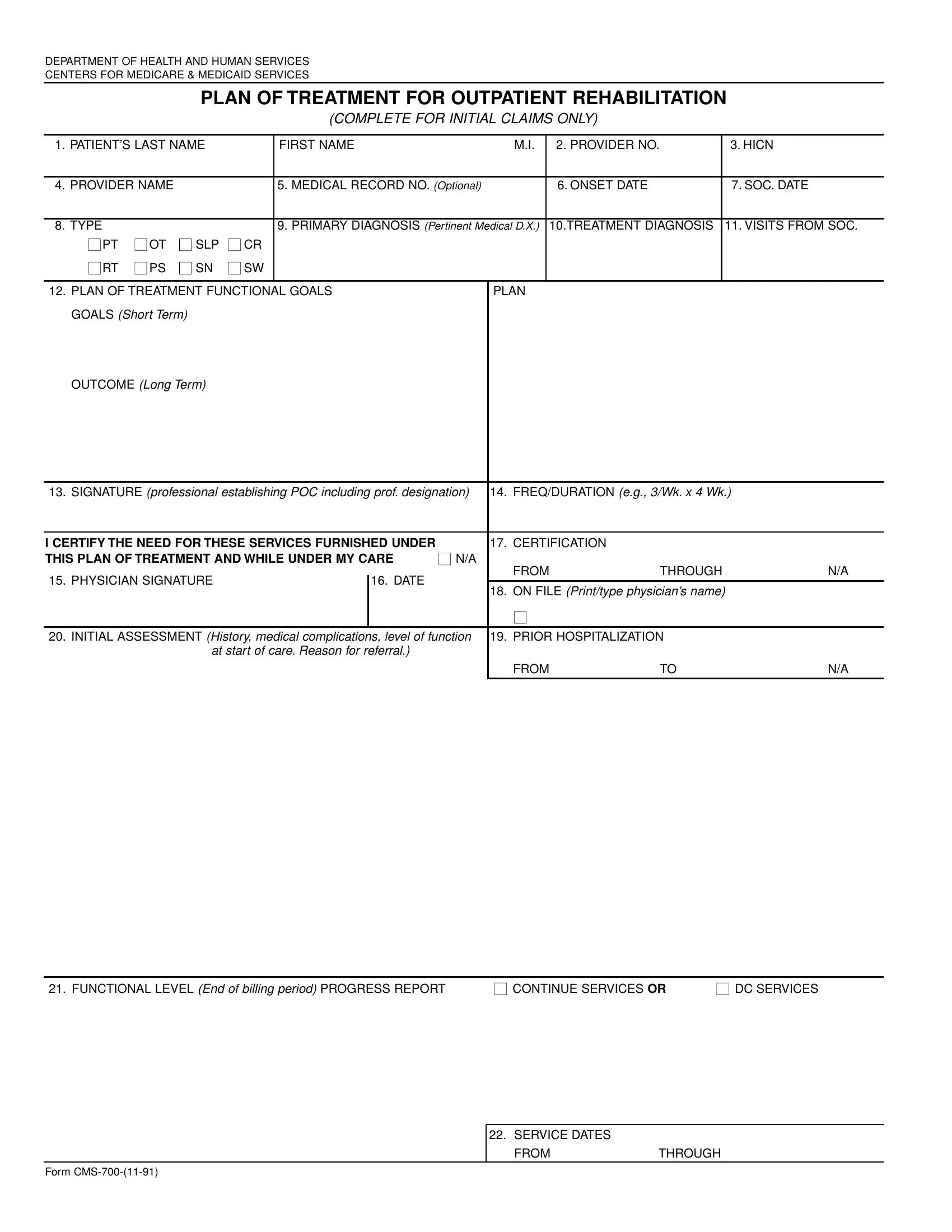
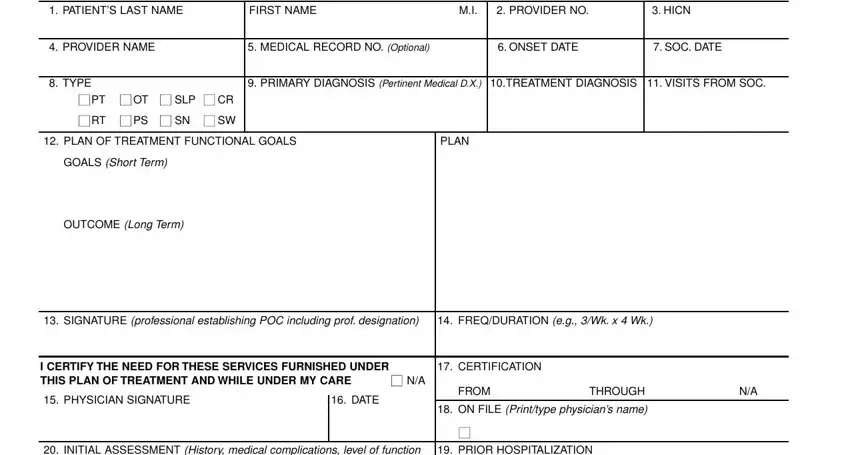
1. The form cms 700 usually requires certain information to be typed in. Be sure that the next fields are filled out:
2. The third step is to fill in the following blank fields: INITIAL ASSESSMENT History, PRIOR HOSPITALIZATION, at start of care Reason for, FROM, FUNCTIONAL LEVEL End of billing, CONTINUE SERVICES OR, and DC SERVICES.
3. This next step is considered rather uncomplicated, Form CMS, SERVICE DATES, FROM, and THROUGH - these form fields will have to be completed here.

Lots of people frequently make some errors when filling in Form CMS in this area. Ensure that you read again what you type in right here.
Step 3: As soon as you've reviewed the details in the file's blanks, click "Done" to complete your form at FormsPal. Sign up with FormsPal right now and easily obtain form cms 700, all set for download. Each and every change you make is handily kept , allowing you to edit the file further if required. FormsPal guarantees your data privacy by using a secure system that never saves or shares any private information provided. Rest assured knowing your files are kept protected whenever you work with our tools!