
You can fill out the Illinois CMS 95 form online for free using the FormsPal PDF editor. The editor works in any browser and does not require software downloads. Follow the steps below to complete this document correctly.
Step 1: Click the "Get Form" button at the top of this page to open the online PDF editor.
Step 2: Use the editor to type your information into each field. You can add text, customize the document, and insert your signature. The editor saves your work in your account so you can return and finish later.
Here is what each section of this form requires:
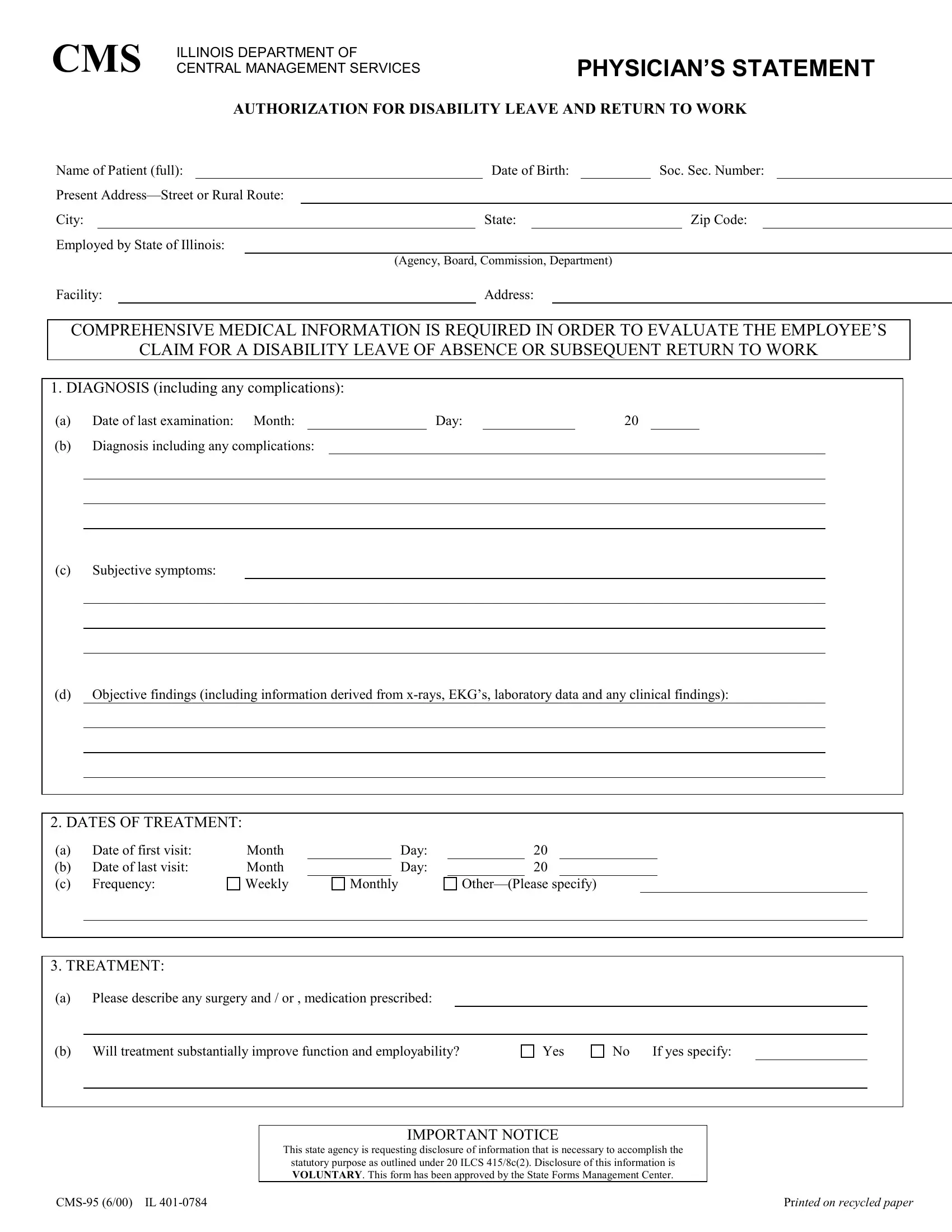
1. Employee and employer information. Enter the employee's full name, home address, and employer name. Make sure this information matches the official records on file with the Illinois Department of Central Management Services. Also include the patient's date of birth, social security number (if required), and department or division.
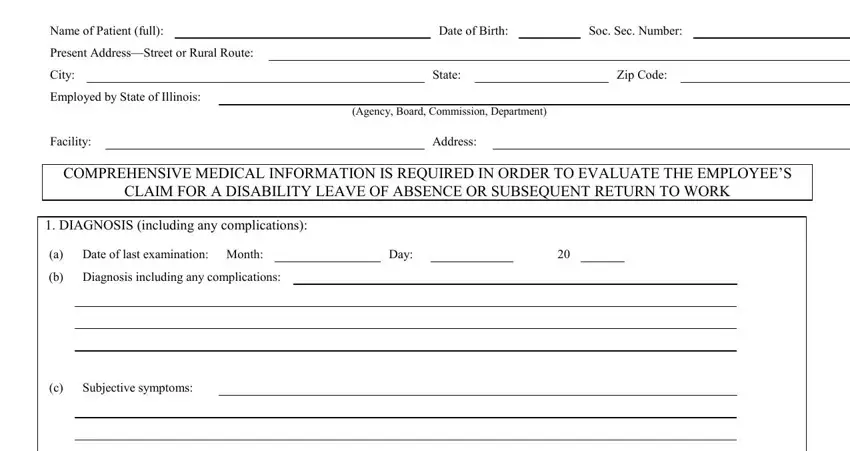
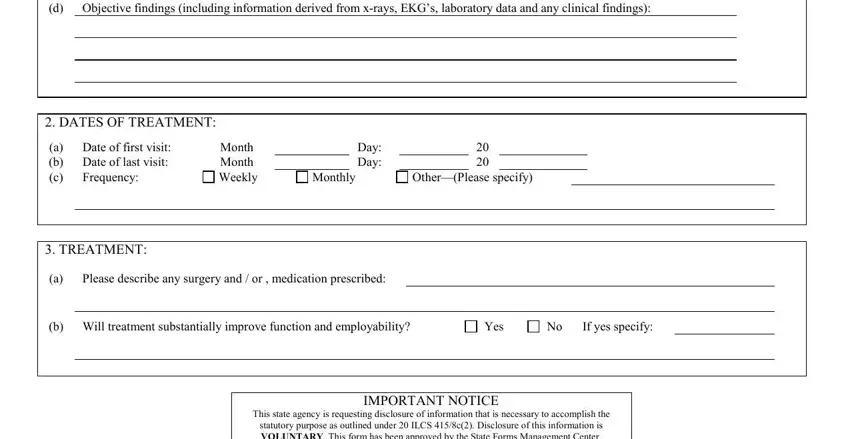
2. Diagnosis and treatment information. Complete the diagnosis, treatment start date, and the date of the most recent visit. Enter how often the patient receives treatment. Note any surgical procedures, including the date and description of surgery. Indicate whether ongoing treatment will significantly change the patient's ability to return to work.
3. Patient progress assessment. Check the box that best describes the patient's current progress: recovered, improved, unchanged, or retrogressed. Indicate whether the patient is ambulatory, house-confined, or bed-confined. If the patient was hospitalized, record the hospital name, address, and the start and end dates of confinement.
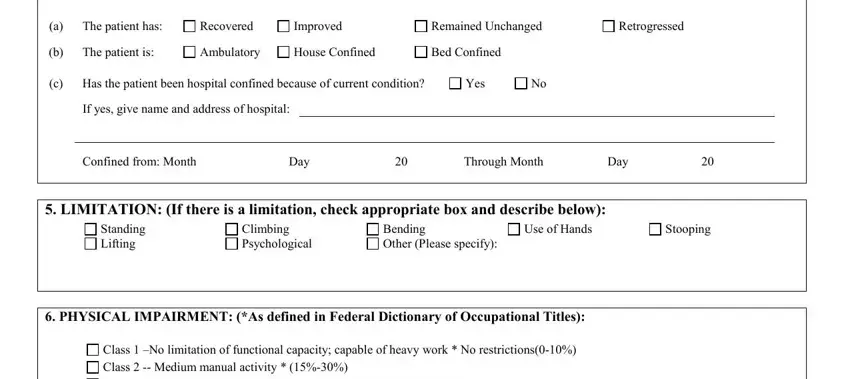
4. Physical impairment and disability extent. Select the appropriate impairment class (Class I through Class V) and add relevant remarks in the space provided. Then complete the disability extent fields, recording whether the patient is disabled from their regular occupation, from any occupation, or both. State your professional opinion on the patient's current ability to work and provide an estimated date of return, if possible.
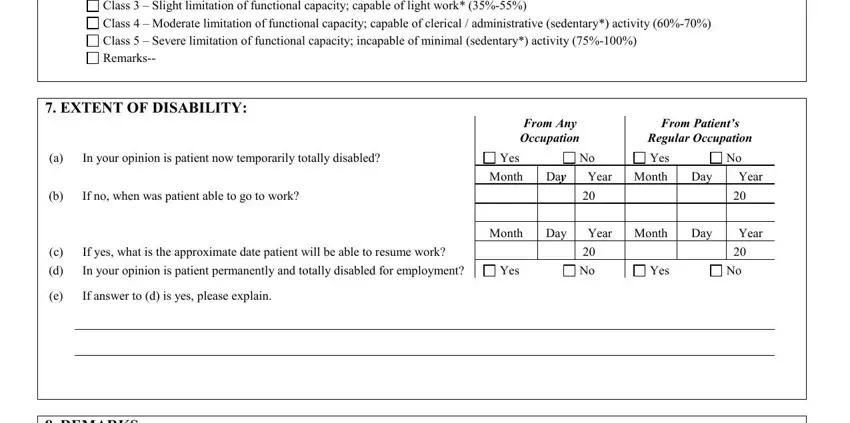
Review the physical impairment section carefully before submitting. Selecting the wrong class can affect the disability benefit determination. Take your time with this section and verify your choice against the patient's current clinical status.
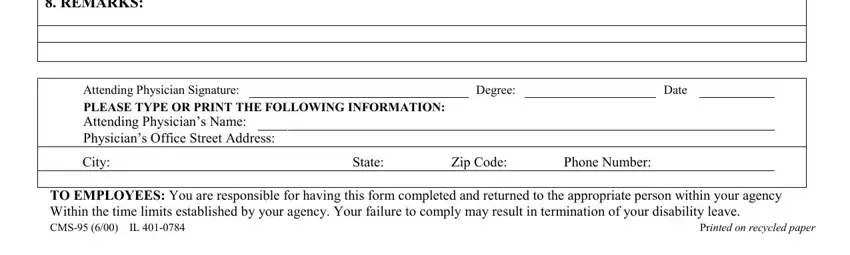
5. Physician certification. The attending physician must print their name and professional degree, sign the form, and enter the date. Provide the office address, city, state, zip code, and phone number. The document will not be processed without a valid physician signature and credentials.
Step 3: Review all information before clicking "Done." Create a free FormsPal account to download the completed document or send it by email. All your saved forms remain in your account for future access. FormsPal uses secure encryption to protect your personal information.
Understanding the impairment classes
The physical impairment section uses a five-class classification system developed to standardize how physicians describe a patient's functional limitations. The Illinois Department of Central Management Services uses this classification to determine disability benefit levels.
Class I: Slight limitation of functional capacity. The patient can perform most activities with minor restriction. This class typically applies when the condition has a minimal effect on day-to-day functioning and most job duties can still be performed.
Class II: Slight limitation of functional capacity for sustained effort. The patient can perform activities for short periods but cannot sustain them over time. This applies when the patient experiences pain or fatigue with prolonged work activity.
Class III: Moderate limitation of functional capacity. The patient can perform some activities with significant restrictions. This classification applies when the condition limits a core function, such as lifting, standing, or sustained concentration, to an extent that prevents regular job performance.
Class IV: Severe limitation of functional capacity. The patient can perform very few activities. This class indicates a need for significant workplace accommodations or an alternate-duty assignment with substantially reduced responsibilities.
Class V: Severe limitation of functional capacity that prevents any productive work. This is the highest level of impairment. A patient in Class V cannot perform any gainful employment during the disability period.
The physician must select the class that accurately reflects the patient's actual functional capacity at the time of the examination. Selecting a class that does not match the clinical evidence may lead to a delay or denial of benefits during the review process.
Tips for completing this form correctly
Use the following guidelines to avoid common processing delays.
Complete every required field. Incomplete submissions are one of the most frequent reasons for processing delays. The physician should fill in all medical sections, including diagnosis, treatment dates, and impairment class. The employee or employer should complete all identification fields at the top.
Use legible writing or the online editor. If you print and fill the form by hand, use black or blue ink. Illegible handwriting can lead to requests for clarification, adding days to the review timeline. The FormsPal editor eliminates this risk by producing clean, typed text.
Double-check the impairment class. This is the most consequential field on the document. Review the patient's current clinical limitations carefully before selecting. Mistakes in this section directly affect the benefit determination.
Keep a copy before submitting. Scan or photocopy the completed document before you send it. If the submission is misplaced or questioned during review, having a copy allows you to respond quickly and re-submit if needed.
Confirm the deadline with HR. Your employer's HR department can tell you the exact submission deadline. Missing this date can reduce or eliminate eligibility for disability benefits during the affected period.
Related forms for Illinois disability leave
This physician's statement is one part of the Illinois state employee disability leave process. Depending on your situation, you may also need:
- FMLA leave form - for federally protected family and medical leave periods
- Leave of absence request form - to formally document a leave request with your employer
- Physician's statement form - for disability or leave programs outside the CMS system
- Return-to-work release form - required when your physician clears you to resume work duties
Frequently asked questions about the CMS 95 form
Who completes this form?
The attending physician completes the medical sections, including the diagnosis, treatment information, impairment class, and physician certification. The employee or employer fills in the personal identification and employment details at the top of the document.
Where do I submit this form?
Submit the completed document to your HR department, who will forward it to the Illinois Department of Central Management Services. Ask your HR contact for the correct submission address or upload portal and the filing deadline.
How long does it take to complete?
Physicians typically spend 15 to 30 minutes on this document. The exact time depends on the complexity of the diagnosis and the level of detail required in the impairment and progress sections.
Can I fill out this form online?
Yes. You can complete this document online using the FormsPal PDF editor. Click "Get Form" at the top of this page, fill in all required fields, and download or print the completed version for submission.
What if my physician makes an error?
For minor errors, the physician should cross out the mistake, write the correct information next to it, and initial the change. Avoid correction fluid. If the error affects the medical opinion or impairment classification, the physician should complete a new form to prevent processing delays.
Does this form need to be notarized?
No. Notarization is not required. The attending physician's signature and professional credentials (degree or license number) serve as the official certification.
Is there a submission deadline?
Yes. The Illinois Department of Central Management Services sets specific deadlines for disability leave documentation. Contact your HR department or the agency directly to confirm current requirements. Late submissions can delay or reduce your disability benefit payments.
Can I use a digital signature?
The FormsPal editor allows you to add a digital signature. However, verify with your employer or the Illinois Department of Central Management Services whether a handwritten signature is required. Some agencies may not accept electronic signatures for disability leave documentation.
How often must the physician complete this form during a leave?
The recertification schedule depends on your employer's requirements and the duration of the leave. In most cases, a new physician's statement is required every 30 to 60 days. Check with your HR department for the specific timeline that applies to your situation.
Is this form required for FMLA leave as well?
The CMS 95 form is specific to the Illinois Department of Central Management Services disability program for state employees. Federal FMLA leave uses different documentation. Ask your HR department whether you also need to complete a FMLA leave form as part of your leave package.