
Getting Started
Open the PDF editor by clicking the "Get Form" button at the top of this page. The editor lets you type directly into all fields, correct existing entries, and attach a digital signature without any software installation. FormsPal uses an encrypted connection and does not store any personal data you enter while working on the document.
Before you begin, gather the following information: the patient's Medicare identification number, the treating therapist's NPI, the ICD-10 diagnosis code for the patient's condition, and the planned frequency and duration of therapy. Having these details ready will allow you to complete the document in a single session.
Step 1: Patient and Provider Information
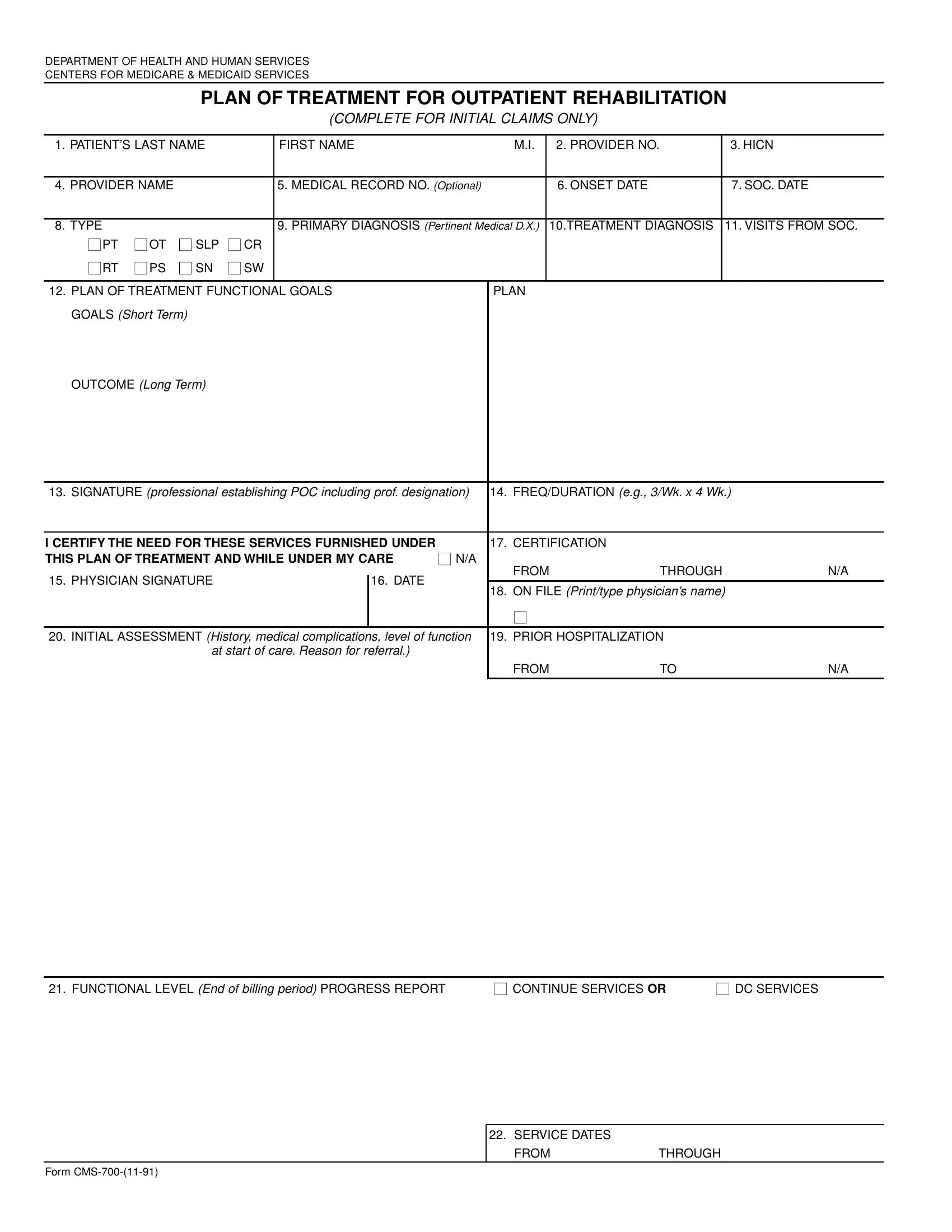
Begin by entering the patient's identifying details at the top of the form. These include the full name and Medicare health insurance claim number, date of birth, and sex. Below that, enter the rendering provider's name, the National Provider Identifier (NPI), and the facility address where therapy services are delivered. Confirm that the facility type matches the outpatient rehabilitation setting noted on the therapist's credentials.
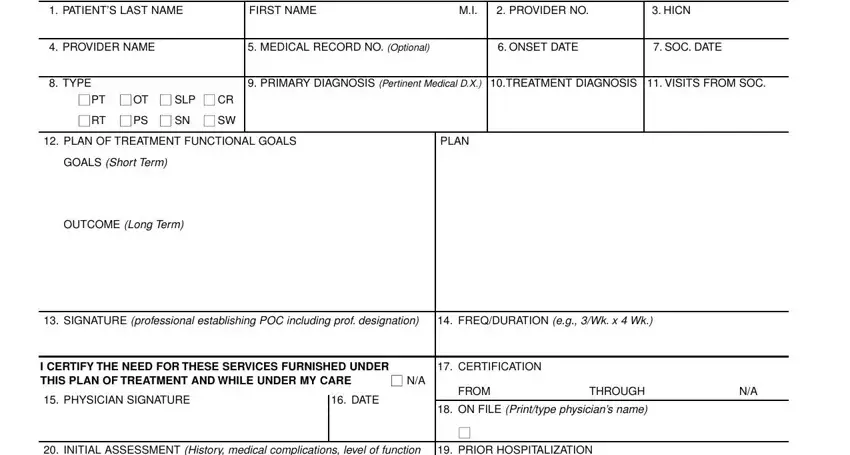
Step 2: Diagnosis, Assessment, and Goals
Enter the ICD-10 diagnosis code that best describes the patient's condition requiring therapy. Record the date of onset and the start-of-care date in the designated fields. In the INITIAL ASSESSMENT History area, summarize the patient's functional limitations and the clinical background that led to the referral for outpatient therapy.
Document PRIOR HOSPITALIZATION dates when the current episode follows a recent inpatient stay, since this context affects the baseline functional level recorded at the start of care. The FUNCTIONAL LEVEL fields need a measurable description of the patient's current abilities and deficits. State goals in objective terms. For example: "Patient will ambulate 150 feet with a standard cane and minimal assistance within six weeks." In the CONTINUE SERVICES OR DC SERVICES block, indicate whether the plan calls for ongoing therapy or discharge at the end of the billing period.
Step 3: Service Dates and Certification
The SERVICE DATES section requires the FROM date and the THROUGH date for the billing period. Verify that these dates match the visit log in the patient's record. The Form CMS identifier and revision date must match the version on file. Review all entries before the physician or qualified non-physician practitioner signs the certification block, because errors in service dates are a leading cause of Medicare claim denials for outpatient therapy providers.

Finishing and Downloading Your Form
After reviewing every field, click "Done" to finalize the document in the FormsPal editor. You can then download the completed PDF, print it for a wet-signature certification, or share it electronically with the supervising physician for countersignature. All changes are saved automatically so you can return to correct any field before the plan is certified and placed in the patient record.
Once the certifying physician has signed, file the original in the patient's medical record and retain a copy for the billing department. If the plan is recertified every 90 days, create a tickler file or calendar reminder to ensure no billing period begins without a current, signed plan on file.
Related Forms for Outpatient Therapy
Outpatient therapy programs often need additional documents alongside the plan of treatment. Chiropractic practices serving Medicare patients use a chiropractic treatment plan form that follows a similar structure for Medicare Part B episodes. Speech-language pathology services are authorized with a speech therapy treatment plan that mirrors the certification process. When a new patient arrives for an initial evaluation, a physical therapy intake form captures the full clinical history before the therapist drafts the plan of treatment.
Frequently Asked Questions
What is the purpose of the CMS 700 form?
It documents the Medicare patient's plan of treatment for outpatient physical, occupational, or speech-language pathology therapy. Medicare requires a signed and dated plan before it reimburses for outpatient rehabilitation services under Part B.
How often must the plan be recertified?
The plan must be initially certified within 30 days of the therapy evaluation and recertified at least every 90 days while the patient continues to receive outpatient rehabilitation services. Missing a recertification deadline can result in claim denials for the uncertified period.
Who signs the plan of treatment?
A physician or qualified non-physician practitioner, such as a physician assistant or nurse practitioner, must review the plan and sign the certification block. The certifying provider must have examined the patient or reviewed pertinent clinical findings in the record before signing.
Can this form be filled out online?
Yes. Open the PDF in the FormsPal editor, complete all required fields, add a signature, and download the finished document. You can then print the signed copy for the certifying physician or share it electronically for countersignature before submitting it with the Medicare claim.