
By using the online editor for PDFs by FormsPal, it is possible to fill out or change cobra letter to employee 2021 right here and now. In order to make our tool better and more convenient to use, we consistently implement new features, considering feedback from our users. All it takes is several simple steps:
Step 1: Simply press the "Get Form Button" at the top of this webpage to launch our pdf form editor. Here you will find everything that is required to work with your file.
Step 2: The editor offers the capability to modify most PDF forms in a variety of ways. Enhance it by adding your own text, adjust existing content, and put in a signature - all close at hand!
It is actually an easy task to complete the pdf with this practical guide! This is what you should do:
1. While completing the cobra letter to employee 2021, make sure to complete all of the needed fields in the corresponding part. It will help to facilitate the process, allowing your information to be handled efficiently and accurately.
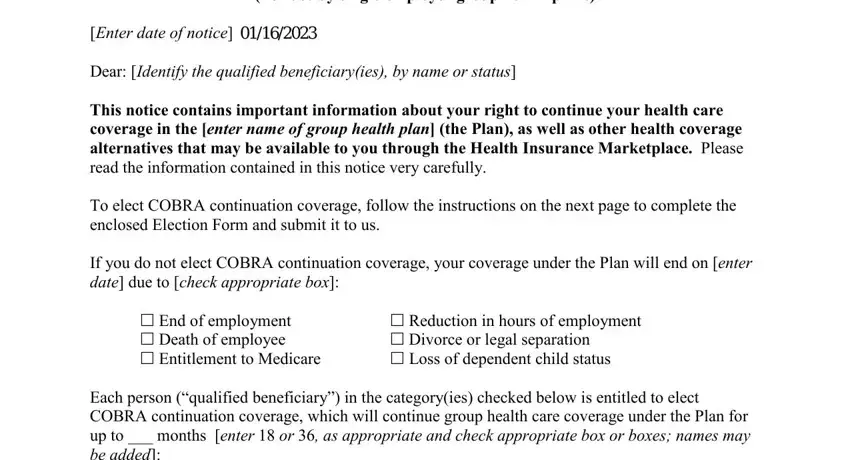
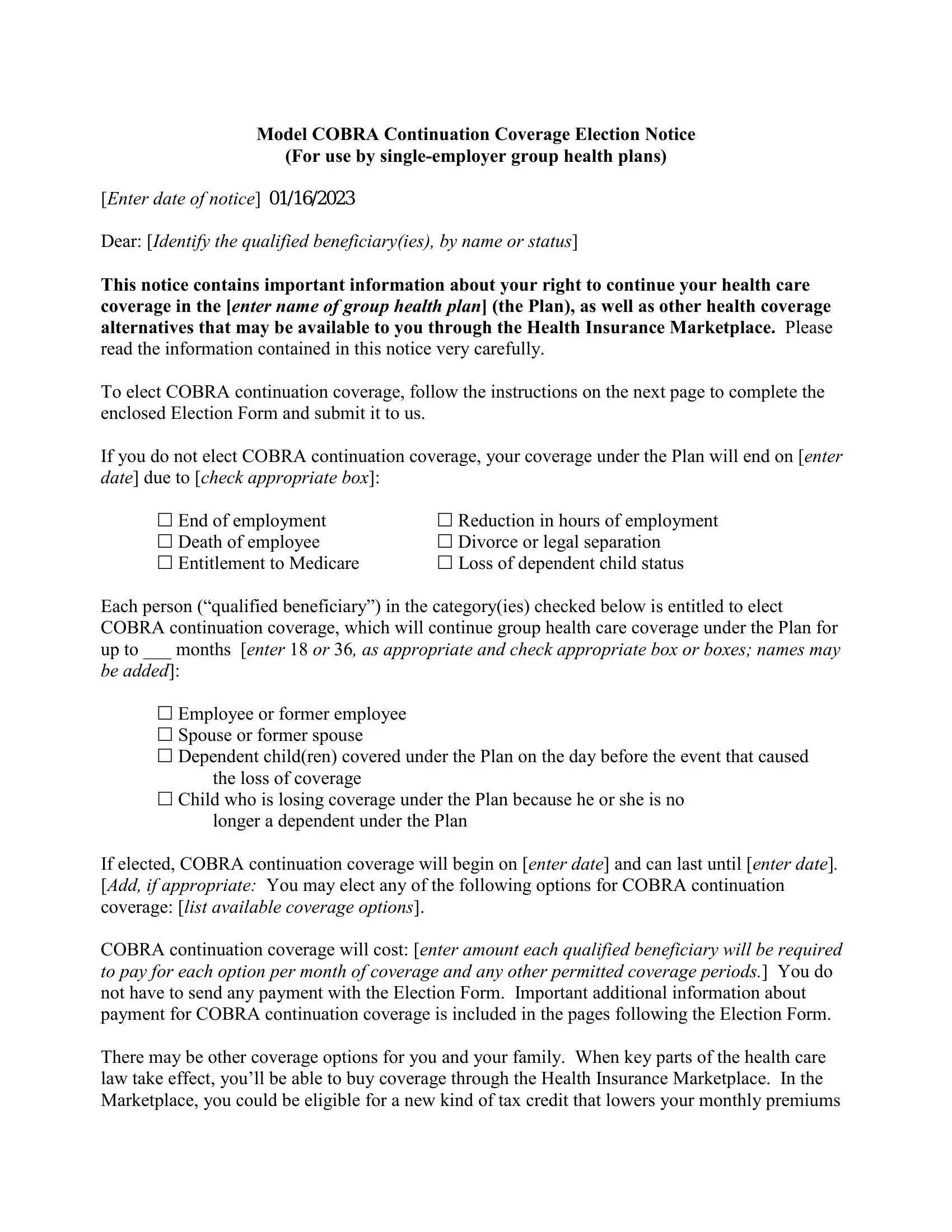
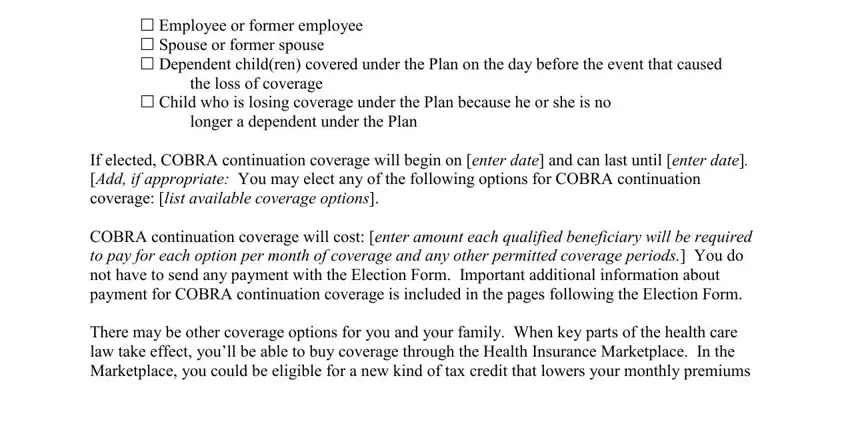
2. Once your current task is complete, take the next step – fill out all of these fields - Enter date of notice Dear Identify, Employee or former employee, the loss of coverage, Child who is losing coverage, longer a dependent under the Plan, and If elected COBRA continuation with their corresponding information. Make sure to double check that everything has been entered correctly before continuing!
Always be very attentive when filling out If elected COBRA continuation and Child who is losing coverage, since this is the section in which most users make some mistakes.
3. This 3rd part should be quite uncomplicated, I We elect COBRA continuation, Add if appropriate Coverage option, Add if appropriate Coverage option, Add if appropriate Coverage option, Signature Print Name, Relationship to individuals, and Date - these form fields needs to be filled out here.
4. This next section requires some additional information. Ensure you complete all the necessary fields - Grace periods for periodic - to proceed further in your process!
Step 3: Be certain that your information is correct and then just click "Done" to finish the project. Go for a free trial plan with us and get direct access to cobra letter to employee 2021 - readily available from your personal account. FormsPal guarantees protected form editing without personal information recording or sharing. Be assured that your details are in good hands here!