
Working with PDF documents online is certainly super easy with our PDF tool. Anyone can fill in colorado driver's license renewal eye exam here with no trouble. Our editor is constantly evolving to grant the very best user experience possible, and that is because of our commitment to continual improvement and listening closely to comments from customers. Here is what you'd need to do to get going:
Step 1: Hit the "Get Form" button above. It is going to open up our tool so you can begin filling in your form.
Step 2: As soon as you open the file editor, you will get the form all set to be completed. Other than filling out different blank fields, you could also do some other actions with the Document, that is writing your own textual content, editing the original text, adding graphics, signing the document, and a lot more.
Be attentive while completing this document. Ensure all mandatory blanks are filled in correctly.
1. It is important to complete the colorado driver's license renewal eye exam correctly, so be mindful while working with the sections including these blank fields:
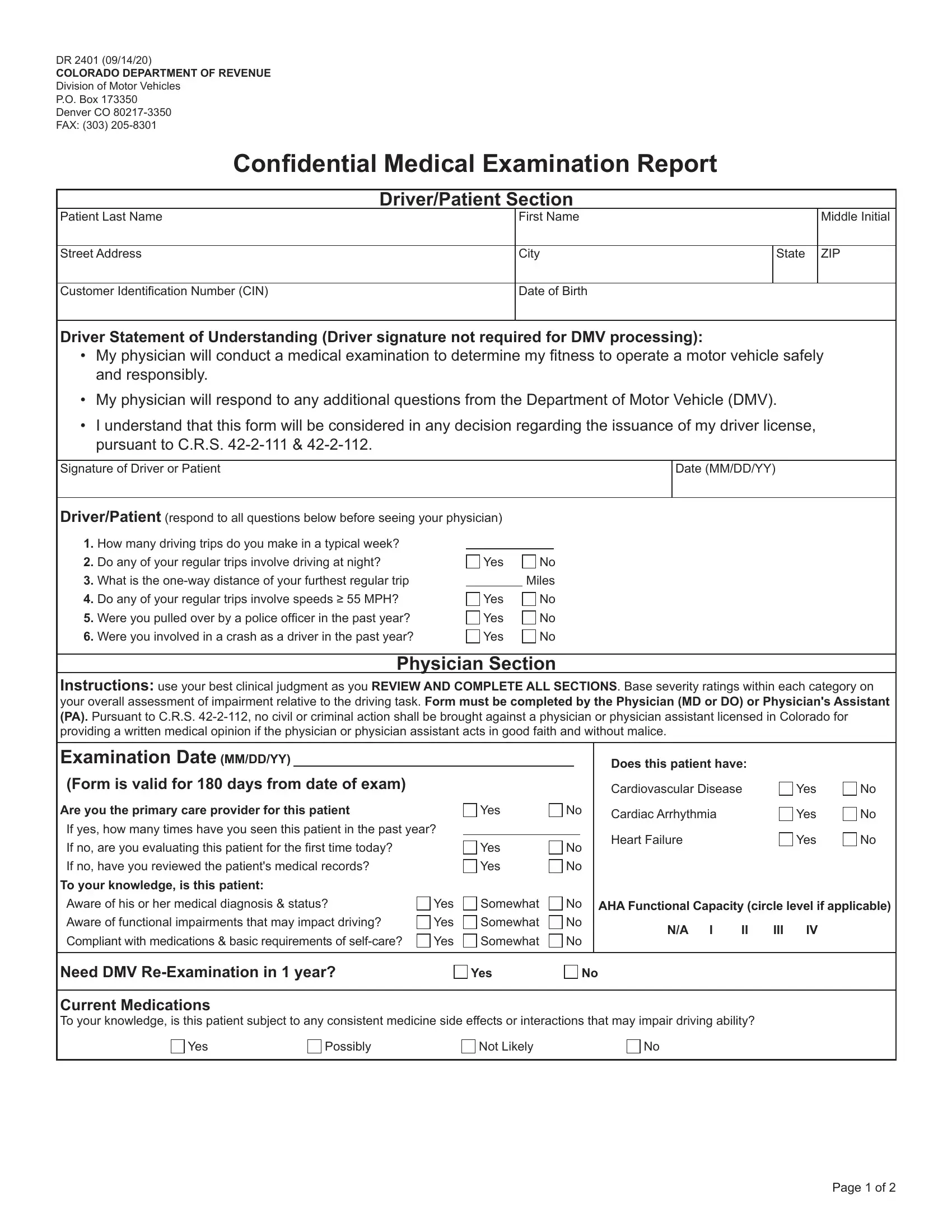
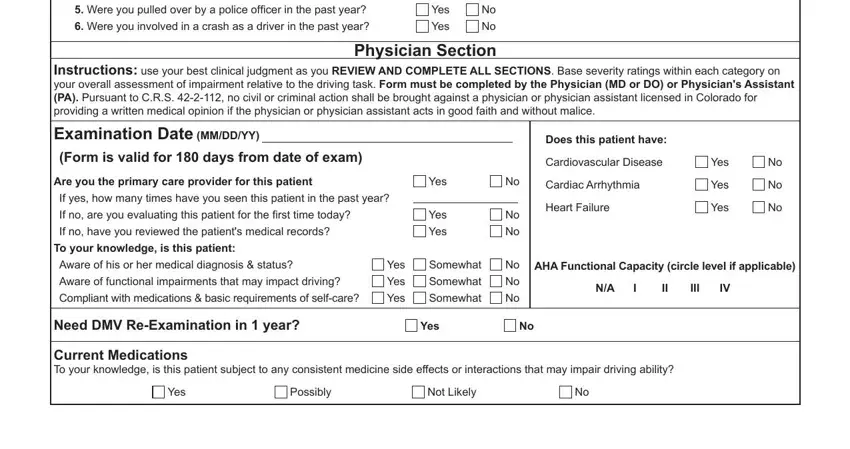
2. When the previous array of fields is finished, you're ready include the needed specifics in What is the oneway distance of, Yes, Yes, Instructions use your best, Physician Section, Examination Date MMDDYY Form is, Yes, Aware of functional impairments, Yes, Yes, Does this patient have, Cardiovascular Disease, Cardiac Arrhythmia, Heart Failure, and Yes allowing you to move on to the 3rd stage.
3. The following step is considered fairly straightforward, Based on my observations of this, Patient Name, Recommended license restrictions, Daylight Driving Only No, Other, Patient Last Name, Must Choose, One, Fit to operate a motor vehicle, medicalfunctional compromise or, Fitness to drive determination, Specialty Required, Patient also requires an eye exam, License Number Required, and Phone Number Required - all of these empty fields needs to be completed here.
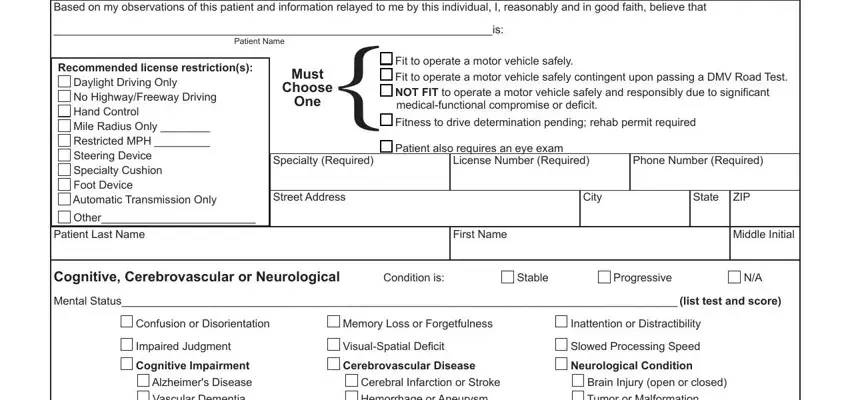
4. The next subsection will require your involvement in the following parts: Impaired Judgment Cognitive, Cerebral Infarction or Stroke, Transient Ischemic Attack, Combined Impairment for Driving, Unimpaired Likely fit to Drive, Carotid Occlusion or Hypoxia, Likely fit to Drive, Questionable Fitness, Condition is, Very Mild, Stable, Mild, Brain Injury open or closed Tumor, Moderate, and Likely Unfit to Drive. Always enter all requested information to go forward.
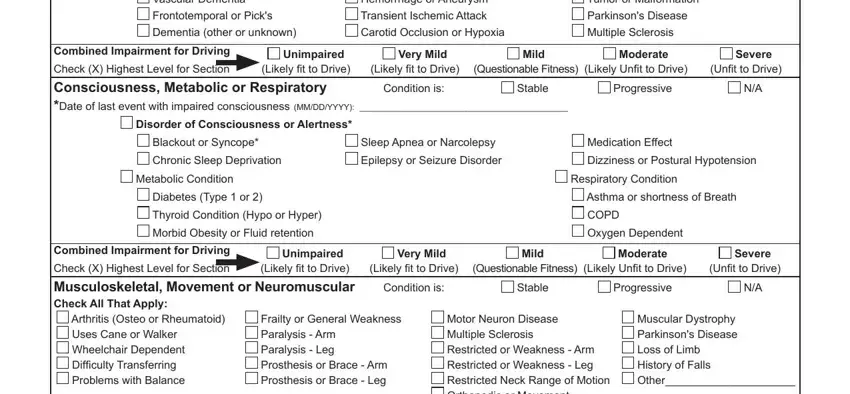
5. To wrap up your form, the last part requires a couple of additional fields. Typing in Combined Impairment for Driving, Unimpaired Likely fit to Drive, Depression, Motor Neuron Disease Multiple, Very Mild, Likely fit to Drive, Condition is, Mild, Questionable Fitness, Moderate, Likely Unfit to Drive, Severe, Unfit to Drive, Stable, and Progressive will conclude the process and you'll be done in a tick!
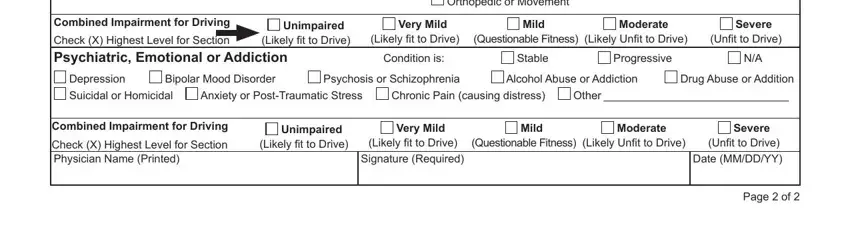
Those who use this PDF generally make some mistakes when filling out Stable in this part. You need to reread everything you enter here.
Step 3: Go through the details you have inserted in the blank fields and then hit the "Done" button. Join FormsPal today and easily get colorado driver's license renewal eye exam, available for download. Every single edit you make is conveniently preserved , making it possible to modify the pdf later on if necessary. We don't sell or share the details that you use whenever filling out documents at FormsPal.