
In case you wish to fill out complaint discrimination federal government, you don't need to download and install any applications - just try our online PDF editor. The tool is continually upgraded by our staff, getting additional features and becoming better. Getting underway is easy! All you should do is adhere to the next basic steps directly below:
Step 1: Click the "Get Form" button above. It'll open up our tool so that you can start completing your form.
Step 2: This editor will allow you to customize your PDF file in a variety of ways. Improve it by writing personalized text, adjust what's already in the PDF, and put in a signature - all doable in no time!
This form will need some specific information; to guarantee accuracy and reliability, you need to heed the subsequent steps:
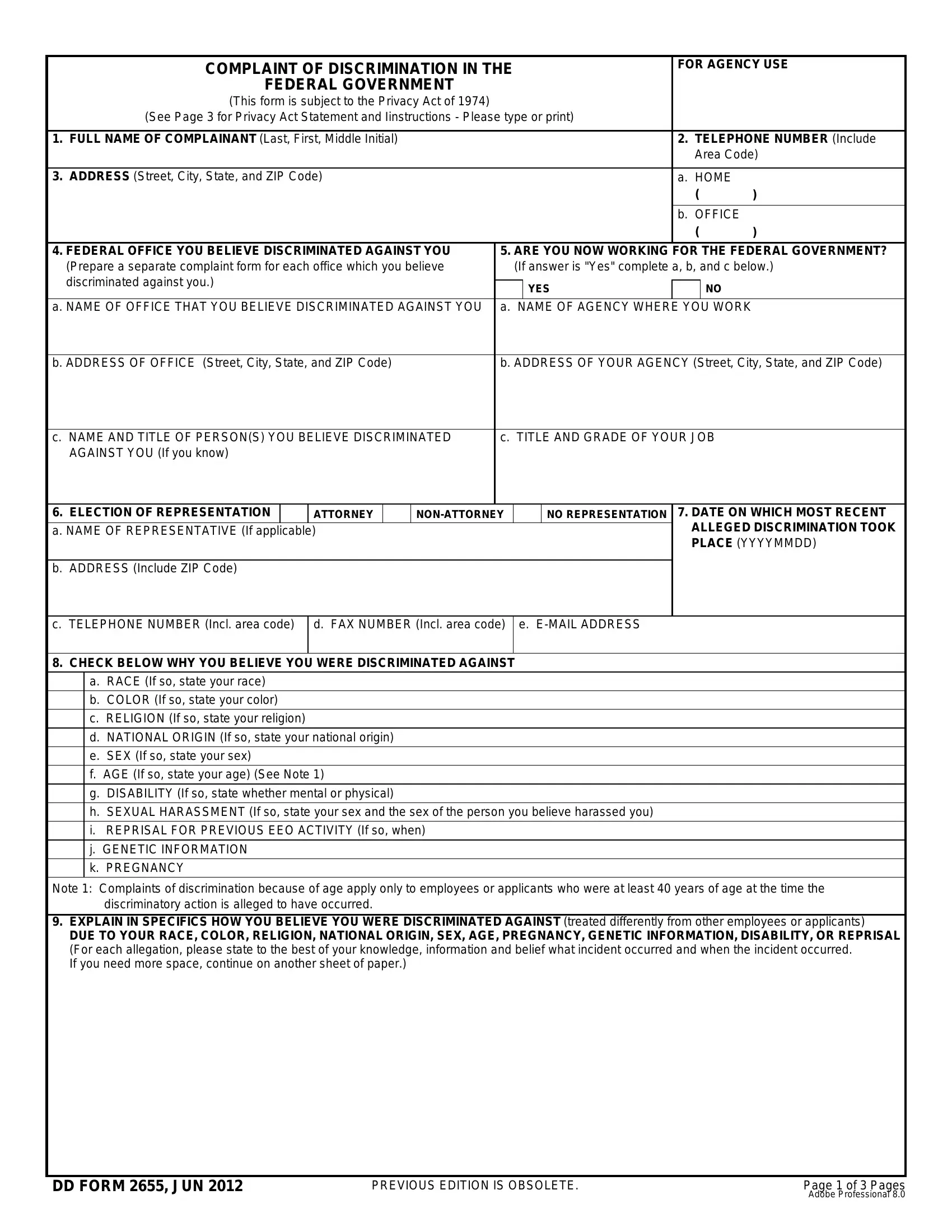
1. Fill out your complaint discrimination federal government with a selection of necessary blank fields. Get all the important information and make certain there is nothing left out!
2. After filling out the last step, head on to the next stage and complete the necessary details in these blank fields - b ADDRESS Include ZIP Code, c TELEPHONE NUMBER Incl area code, d FAX NUMBER Incl area code e, CHECK BELOW WHY YOU BELIEVE YOU, a RACE If so state your race b, and Note Complaints of discrimination.
3. This next segment is focused on I HAVE DISCUSSED MY COMPLAINT, NAME OF COUNSELOR If applicable, YES, HAVE THE ISSUES IDENTIFIED IN, YES If Yes complete a b and c below, a X one MSPB, UNION NEGOTIATED GRIEVANCE, b DATE FILED YYYYMMDD, c MSPB OR UNION DOCKET NUMBER If, and WHAT RELIEF ARE YOU SEEKING TO - complete every one of these fields.
4. To move ahead, the next step will require completing a couple of form blanks. Examples of these are LIST NAMES OF WITNESSES AND, which you'll find crucial to continuing with this process.

Be extremely mindful when completing LIST NAMES OF WITNESSES AND and LIST NAMES OF WITNESSES AND, since this is the section where a lot of people make errors.
5. To wrap up your document, this last segment incorporates some extra fields. Entering SIGNATURE OF COMPLAINANT, DD FORM JUN, DATE OF THIS COMPLAINT YYYYMMDD, and Page of Pages is going to wrap up everything and you will be done in a tick!

Step 3: Before submitting your form, make certain that all form fields have been filled out right. Once you’re satisfied with it, click “Done." Create a 7-day free trial option with us and obtain instant access to complaint discrimination federal government - with all transformations preserved and available from your personal cabinet. With FormsPal, you can easily complete forms without being concerned about personal information breaches or data entries getting shared. Our secure software ensures that your personal data is stored safely.