Are you unsatisfied with a product or service that you have received from Mcad? If so, then your first step should be to file a formal complaint using the Mcad Complaint Form. This form allows consumers to quickly and easily document their issues with a product or service they have bought in order to receive restitution. When filling out the form, it is important to provide as much detail as possible so that your issue can be resolved in an effective manner by the Mcad team. In this blog post, we will discuss what information you need to include on the complaint form, how to submit it, and what further action steps can take afterwards.
| Question | Answer |
|---|---|
| Form Name | Mcad Complaint Form |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | mcad comnplaint form, mcad complaint sample, complaint form mcad, mcad omplaint process |
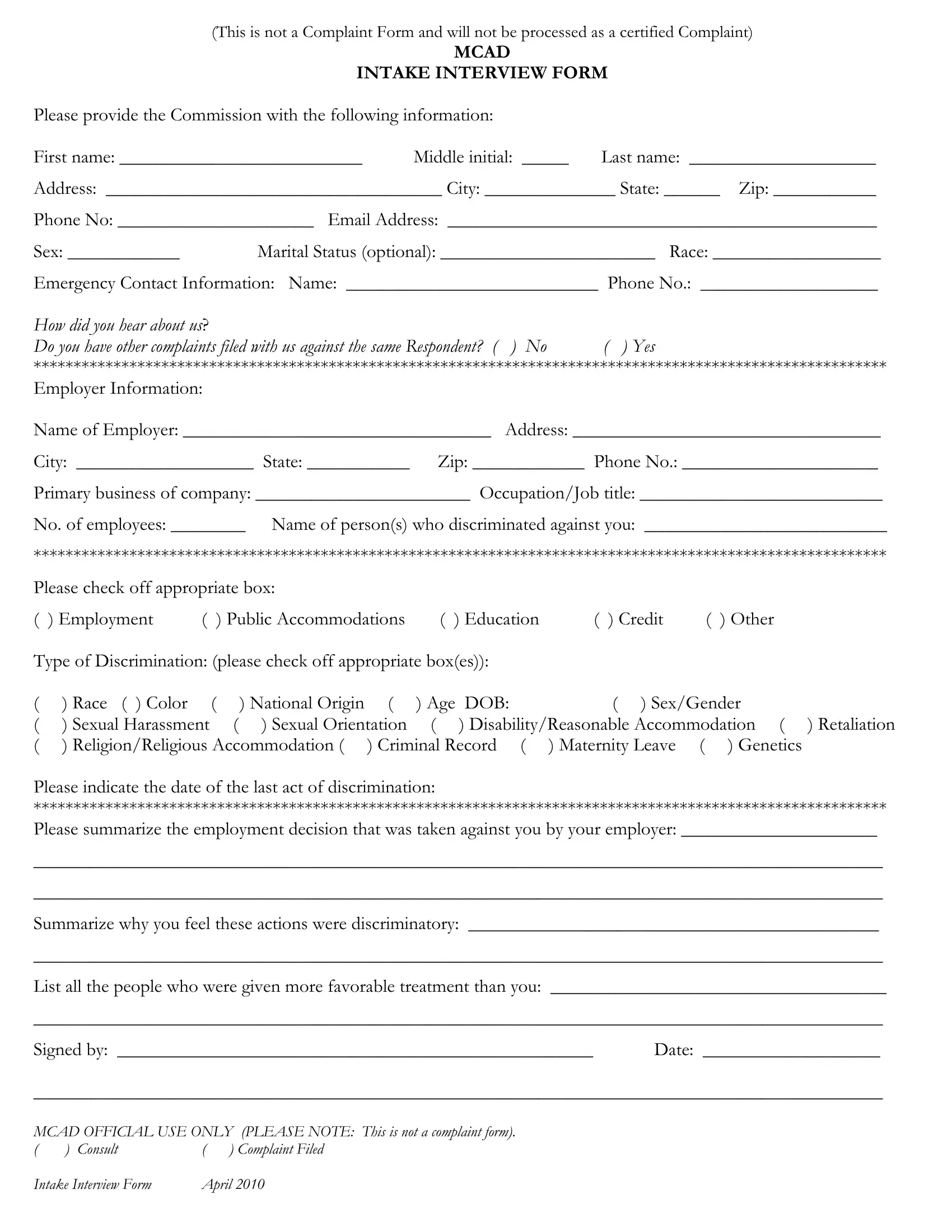
(This is not a Complaint Form and will not be processed as a certified Complaint)
MCAD
INTAKE INTERVIEW FORM
Please provide the Commission with the following information:
First name: __________________________ Middle initial: _____ Last name: ____________________
Address: ____________________________________ City: ______________ State: ______ Zip: ___________
Phone No: _____________________ Email Address: ______________________________________________
Sex: ____________ Marital Status (optional): _______________________ Race: __________________
Emergency Contact Information: Name: ___________________________ Phone No.: ___________________
How did you hear about us?
Do you have other complaints filed with us against the same Respondent? ( ) No ( ) Yes
***********************************************************************************************************
Employer Information:
Name of Employer: _________________________________ Address: _________________________________
City: ___________________ State: ___________ Zip: ____________ Phone No.: _____________________
Primary business of company: _______________________ Occupation/Job title: __________________________
No. of employees: ________ Name of person(s) who discriminated against you: __________________________
***********************************************************************************************************
Please check off appropriate box: |
|
|
|
|
( ) Employment |
( ) Public Accommodations |
( ) Education |
( ) Credit |
( ) Other |
Type of Discrimination: (please check off appropriate box(es)):
( |
) Race ( ) Color |
( |
) National Origin ( |
) Age |
DOB: |
( ) Sex/Gender |
( |
) Sexual Harassment |
( |
) Sexual Orientation |
( |
) Disability/Reasonable Accommodation ( ) Retaliation |
|
() Religion/Religious Accommodation ( ) Criminal Record ( ) Maternity Leave ( ) Genetics
Please indicate the date of the last act of discrimination:
***********************************************************************************************************
Please summarize the employment decision that was taken against you by your employer: _____________________
___________________________________________________________________________________________
___________________________________________________________________________________________
Summarize why you feel these actions were discriminatory: ____________________________________________
___________________________________________________________________________________________
List all the people who were given more favorable treatment than you: ____________________________________
___________________________________________________________________________________________
Signed by: ___________________________________________________ Date: ___________________
___________________________________________________________________________________________
MCAD OFFICIAL USE ONLY (PLEASE NOTE: This is not a complaint form).
( |
) Consult |
( |
) Complaint Filed |
Intake Interview Form |
April 2010 |