
With the online editor for PDFs by FormsPal, it is possible to fill in or edit cs 205 b right here and now. Our tool is consistently developing to deliver the very best user experience possible, and that is thanks to our resolve for constant enhancement and listening closely to comments from customers. It just takes several easy steps:
Step 1: Open the CS-205 B Form Editor
Click the "Get Form Button" at the top of this site to open our PDF form editing tool. Here you will find everything that is required to fill out your file.
Step 2: Review the Editing Options
Once you start the editor, you will see the document made ready to be completed. Besides filling in different blank fields, it is also possible to do some other things with the form, namely writing any textual content, modifying the initial text, inserting illustrations or photos, placing your signature to the PDF, and much more.
With regards to the blank fields of this specific form, here is what you should know:
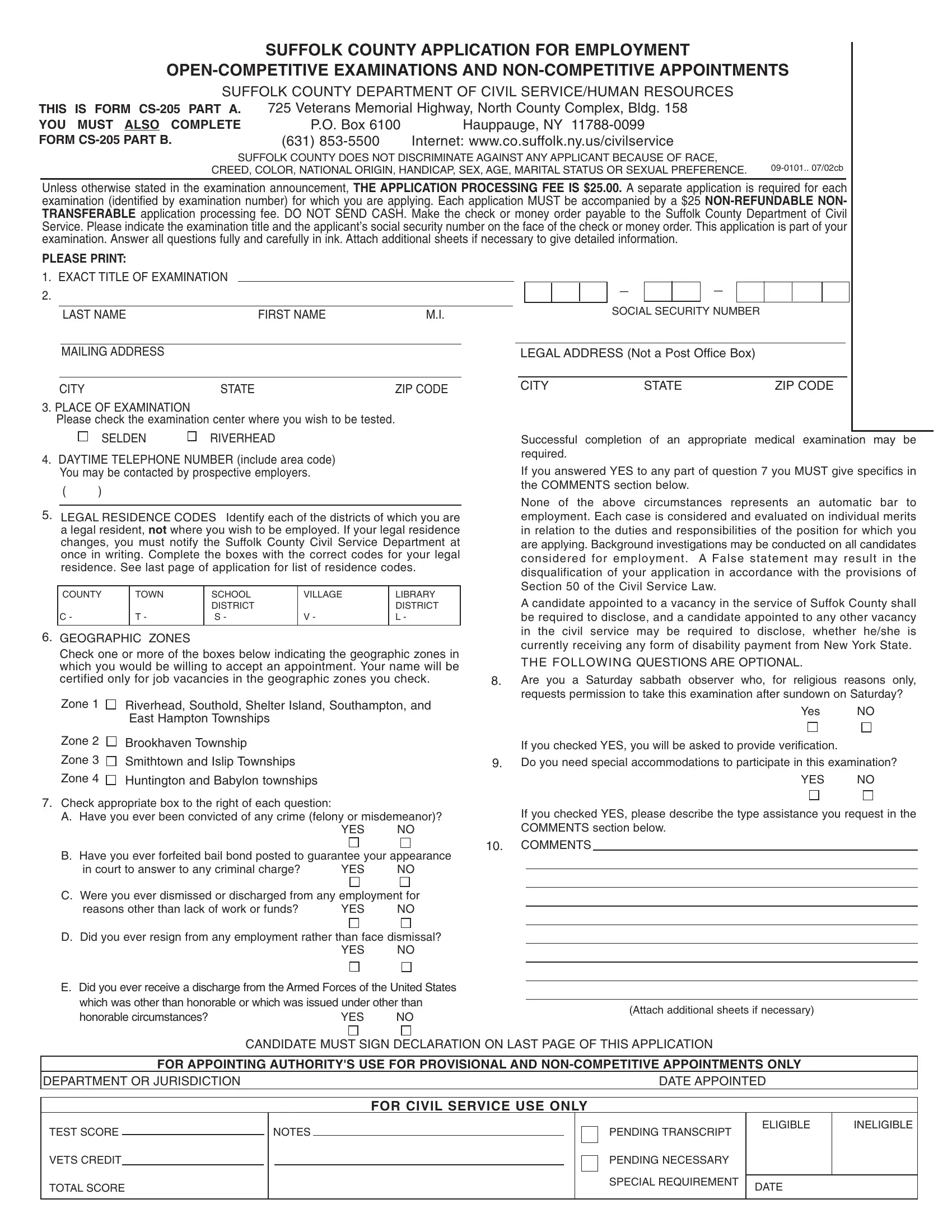
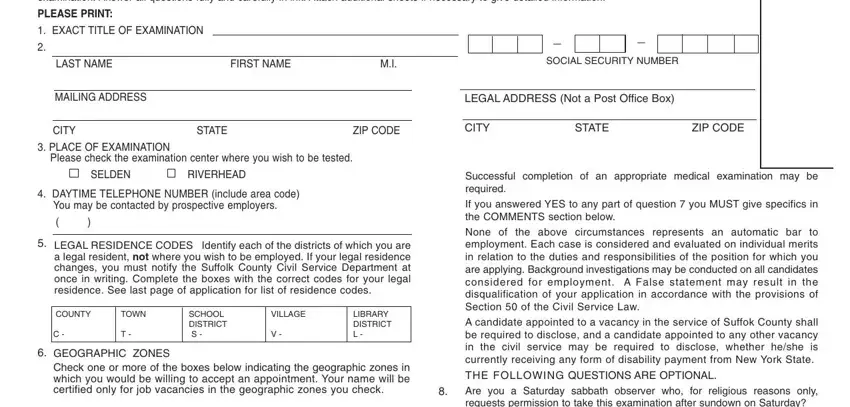
Section 1: Personal Information and Zone Selection
1. You should complete the cs 205 b correctly, hence be attentive while filling out the segments that contain all of these fields:
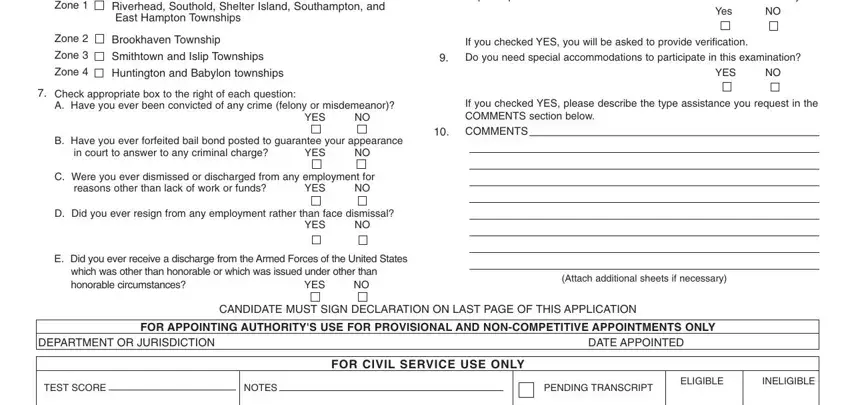
Section 2: Legal History and Background Questions
2. After this section is complete, you are ready to include the needed details in Zone, Zone, Zone, Zone, Riverhead Southold Shelter Island, Brookhaven Township, Smithtown and Islip Townships, Huntington and Babylon townships, Check appropriate box to the right, YES, B Have you ever forfeited bail, in court to answer to any criminal, YES, C Were you ever dismissed or, and reasons other than lack of work or so you can move forward further.
Section 3: Education and Eligibility Requirements
3. Your next stage is normally easy - fill in all of the form fields in YOUR ELIGIBILITY TO COMPETE IN, EDUCATION, A Have you graduated from senior, YES, If yes complete name and location, Name of school, Location, If you have a high school, Issuing Authority, If you did NOT graduate from high, PLEASE ATTACH A COPY OF COLLEGE, Full Name of School, StateCity in which located, Dates of Attendance, and Month and Year in order to complete this segment.
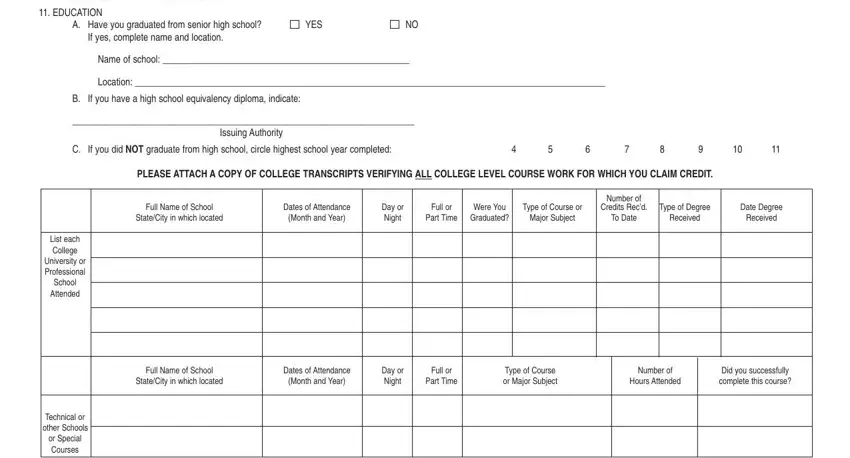
When it comes to Month and Year and Name of school, ensure that you review things here. Both of these are surely the most significant ones in the PDF.
Section 4: Driver License, Professional Licenses, and Work Experience
4. Filling out DRIVERS LICENSE Circle the class, E M, Date of Expiration, LICENSES If a license certificate, Name of Trade or Profession, License Number, Granted by licensing agency, City or State, Specialty, Date License First Issued, Registered From, DESCRIPTION OF EXPERIENCE, Beginning with the most recent, ALL EXPERIENCE IS SUBJECT TO, and LENGTH OF EMPLOYMENT is key in this section - make sure you take the time and fill out each and every blank area!
Section 5: Final Employment Details
5. Since you come close to the completion of this form, there are actually a few extra things to do. Specifically, WK MO YR, TYPE OF BUSINESS, YOUR EXACT TITLE, Average no of hrs worked per week, SUPERVISORS TITLE, SUPERVISORS NAME, and TELEPHONE NUMBER should all be done.
Step 3: Save and Download Your Completed CS-205 B Form
Confirm that your information is accurate and then press "Done" to finish the project. After creating a free trial account here, you will be able to download cs 205 b or send it via email promptly. The file will also be easily accessible in your personal account with your every change. We do not sell or share the information you type in whenever filling out forms at our website.
Common Mistakes to Avoid on the CS-205 B Form
Applicants frequently miss listing all prior employment or leave out the supervisor name and contact details. Double-check that your educational credentials match exactly what is listed on your diploma or transcript. Geographic zone selection is required and must reflect where you are willing to work. Omitting the application fee or submitting an incorrect amount will result in a delayed or rejected application.
Related Civil Service and Employment Application Forms
If you need additional civil service forms or general employment applications, the following resources on FormsPal may be helpful:
- Civil Service 55-B Form - Used for open-competitive civil service hiring in New York
- Ohio Civil Service Application - Standard employment application for Ohio state and local government positions
- General Employment Application Form - A comprehensive job application template for various employers