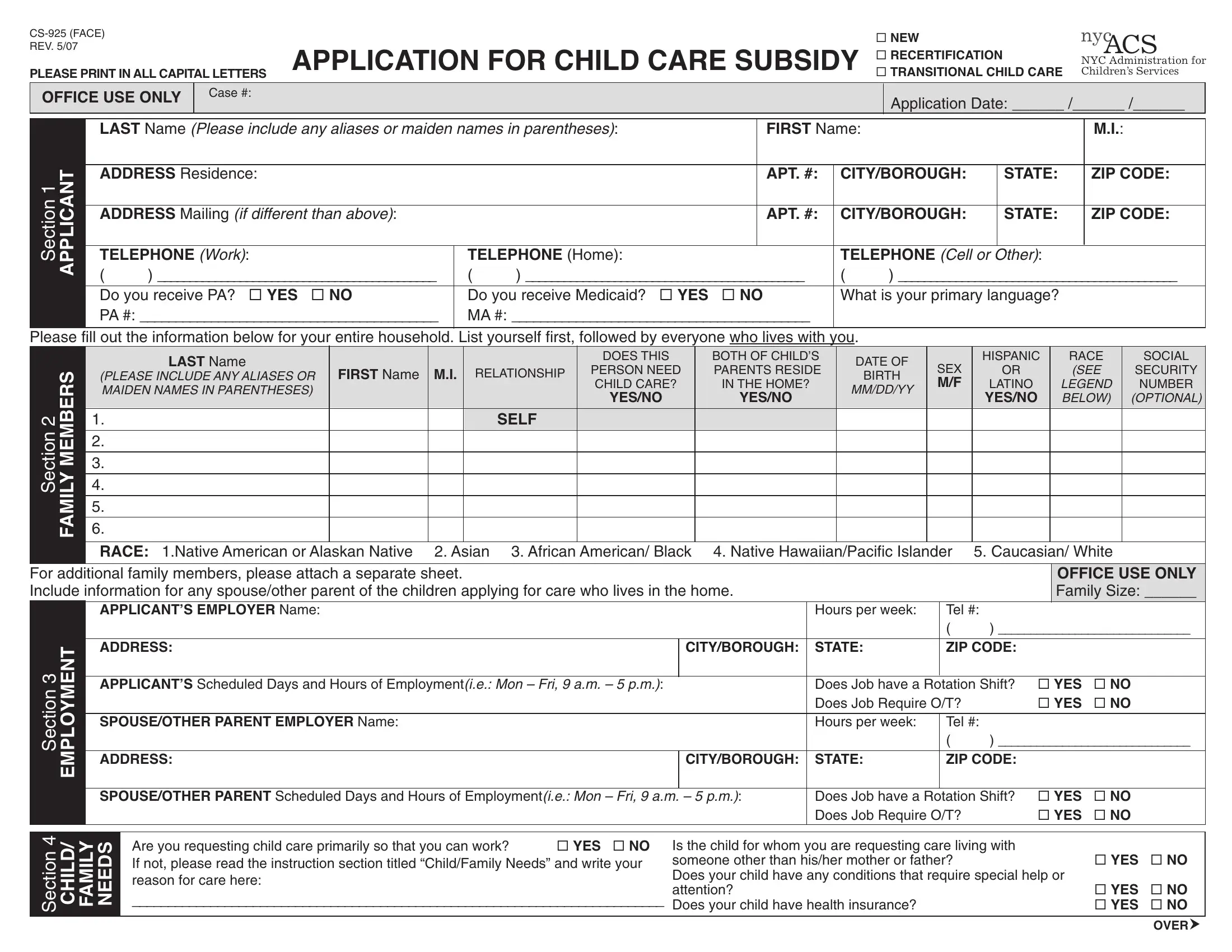
The CS-925 form is the official NYC Administration for Children's Services (ACS) application for child care subsidy assistance. Families in New York City can use this form to request financial help for child care when a parent or guardian is working, attending school, or enrolled in an approved job training program.
The form requires detailed information about the applicant's household, employment status, income, and the child care needs of the family. Parents and guardians must provide personal data including full name (with any aliases or maiden names), home address, and contact number. The form also asks about each household member, particularly the children for whom child care is requested.
The employment section of the CS-925 form asks applicants to list their employer's name and address, weekly work hours, schedule type, and any overtime or rotating shifts. This information helps ACS determine eligibility for child care subsidy based on the family's work or education status.
Applicants must also declare all sources of household income and provide documentation for verification. ACS uses this information to assess financial eligibility for the child care assistance program. The form allows families to specify a preferred child care provider and the type of care needed, such as center-based care, family day care, Head Start, or informal care arrangements.
By signing the completed CS-925 form, applicants confirm that all information is accurate and acknowledge the legal consequences of falsifying information. This form is a required step in obtaining a child care subsidy in New York City.
| Question | Answer |
|---|---|
| Form Name | CS 925 Form |
| Also Known As | NYC ACS Child Care Subsidy Application |
| Issuing Agency | Administration for Children's Services (ACS) |
| City / State | New York City, NY |
| Form Length | 2 pages |
| Purpose | Child care subsidy application |
| Fillable? | No |
| Avg. time to fill out | 30 min |
| Other names | CS-925, RECERTIFICATION, TANF, ACS |