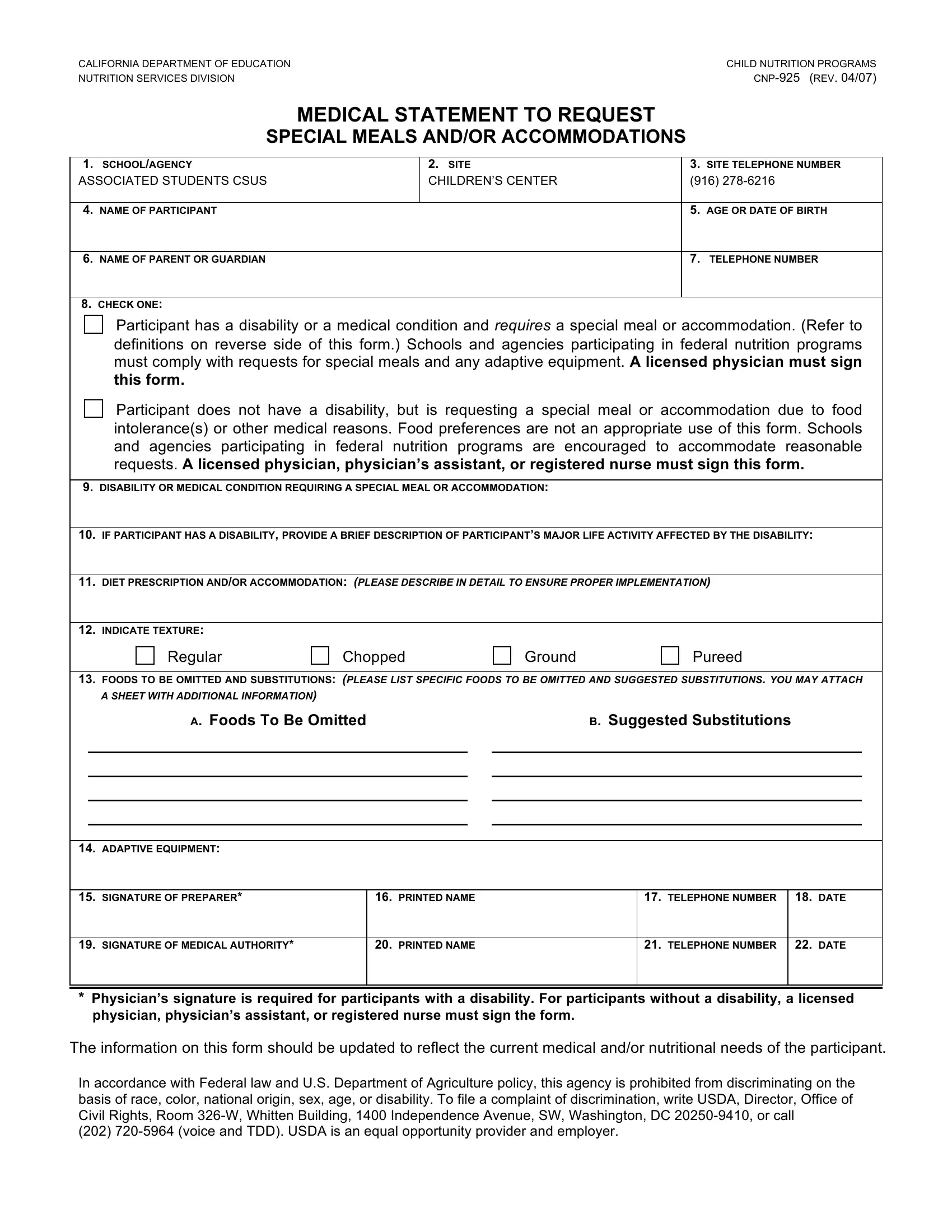
Ensuring that all children and adults participating in federal nutrition programs have their dietary needs met is a priority that is taken very seriously. The CNP-925 form, crafted by the California Department of Education's Nutrition Services Division, is a crucial tool designed to facilitate this process. This form serves as a medical statement, enabling requests for special meals and/or accommodations to be formally made for individuals with either a disability that affects their diet or a medical condition that necessitates a specific dietary protocol. These accommodations can range from texture modifications like pureed or chopped foods to the complete omission of certain allergens, as well as the necessary adaptive equipment to assist the participant while eating. The completion and signing of this form by a licensed physician, or in the case of non-disability-related requests, a physician’s assistant or registered nurse, are essential steps to ensuring these dietary needs are officially recognized and catered to. Moreover, this process not only underscores the inclusive approach of educational and childcare institutions towards nutritional care but also aligns with federal non-discrimination laws, embodying a commitment to provide equal opportunities and support for all participants in nutrition programs.
| Question | Answer |
|---|---|
| Form Name | Form Cnp 925 |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | TDD, 326-W, cnp 925 form new, hemic |
