
In case you want to fill out cto form, you don't need to download any kind of software - just try using our online PDF editor. To make our editor better and less complicated to use, we consistently develop new features, bearing in mind suggestions coming from our users. This is what you would need to do to get going:
Step 1: First, access the tool by pressing the "Get Form Button" at the top of this page.
Step 2: This editor grants the capability to modify PDF documents in various ways. Modify it by adding customized text, correct existing content, and add a signature - all doable within minutes!
This document will need particular information to be typed in, thus you should definitely take your time to enter what is requested:
1. Whenever filling out the cto form, ensure to include all essential blanks in the corresponding section. This will help to facilitate the work, making it possible for your information to be handled swiftly and appropriately.
2. After filling in this section, head on to the next part and fill in all required particulars in these blank fields - Patient Details, CHI Number, Surname, First Name s, Other Known As, Title, DoB dd mm yyyy, Other Known As could include any, Medical Practitioner Details, Note Where an examination is, Surname, First Name, Title, and Address.
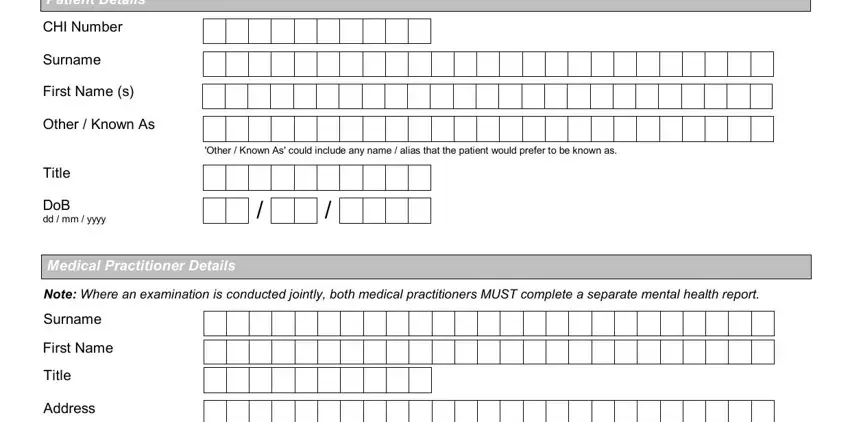
Concerning Note Where an examination is and Title, ensure that you do everything correctly in this section. Both of these are certainly the most significant fields in the PDF.
3. The following segment will be focused on Postcode, Telephone, email address, CTO v, and Page of - complete each one of these blank fields.
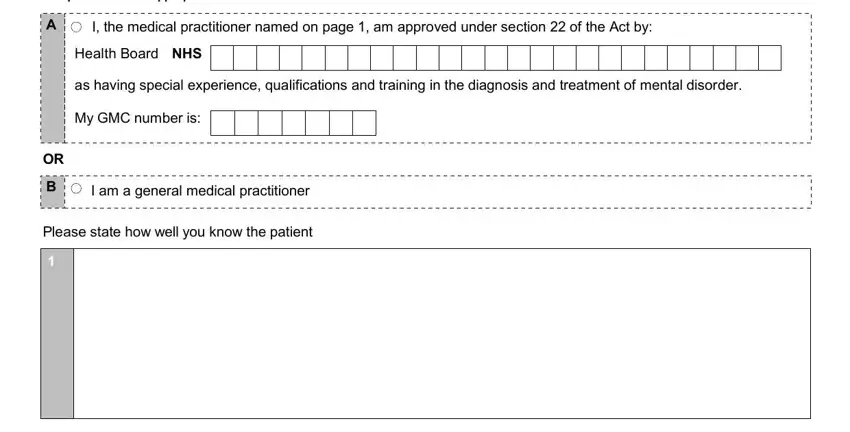
4. This next section requires some additional information. Ensure you complete all the necessary fields - Complete A or B as appropriate, I the medical practitioner named, Health Board NHS, as having special experience, My GMC number is, I am a general medical practitioner, and Please state how well you know the - to proceed further in your process!
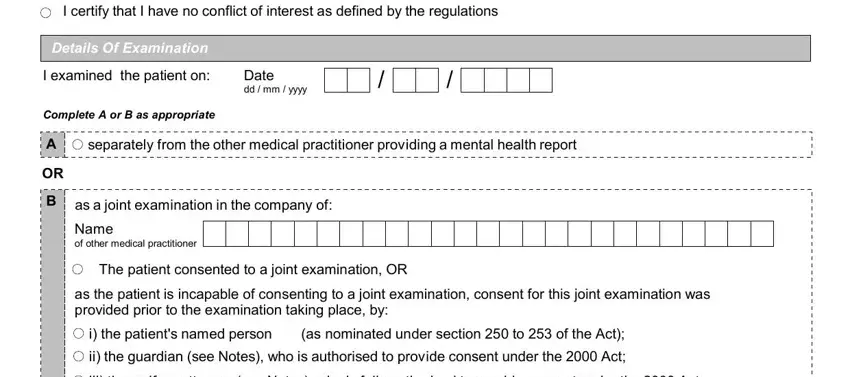
5. When you come near to the end of your file, you'll find a couple more things to undertake. Notably, I certify that I have no conflict, Details Of Examination, I examined the patient on, Complete A or B as appropriate, Date dd mm yyyy, separately from the other medical, B as a joint examination in the, Name of other medical practitioner, The patient consented to a joint, as the patient is incapable of, i the patients named person, as nominated under section to of, ii the guardian see Notes who is, and iii the welfare attorney see Notes should all be filled out.
Step 3: Before moving forward, ensure that blanks have been filled in the proper way. As soon as you’re satisfied with it, click “Done." Try a free trial subscription with us and get direct access to cto form - downloadable, emailable, and editable from your personal cabinet. At FormsPal.com, we do our utmost to make sure that your information is maintained protected.