
Filing an SSS benefit claim requires advance preparation. Follow these steps to complete the form accurately and gather the correct documents before visiting a branch.
How to Fill Out the Form Step by Step
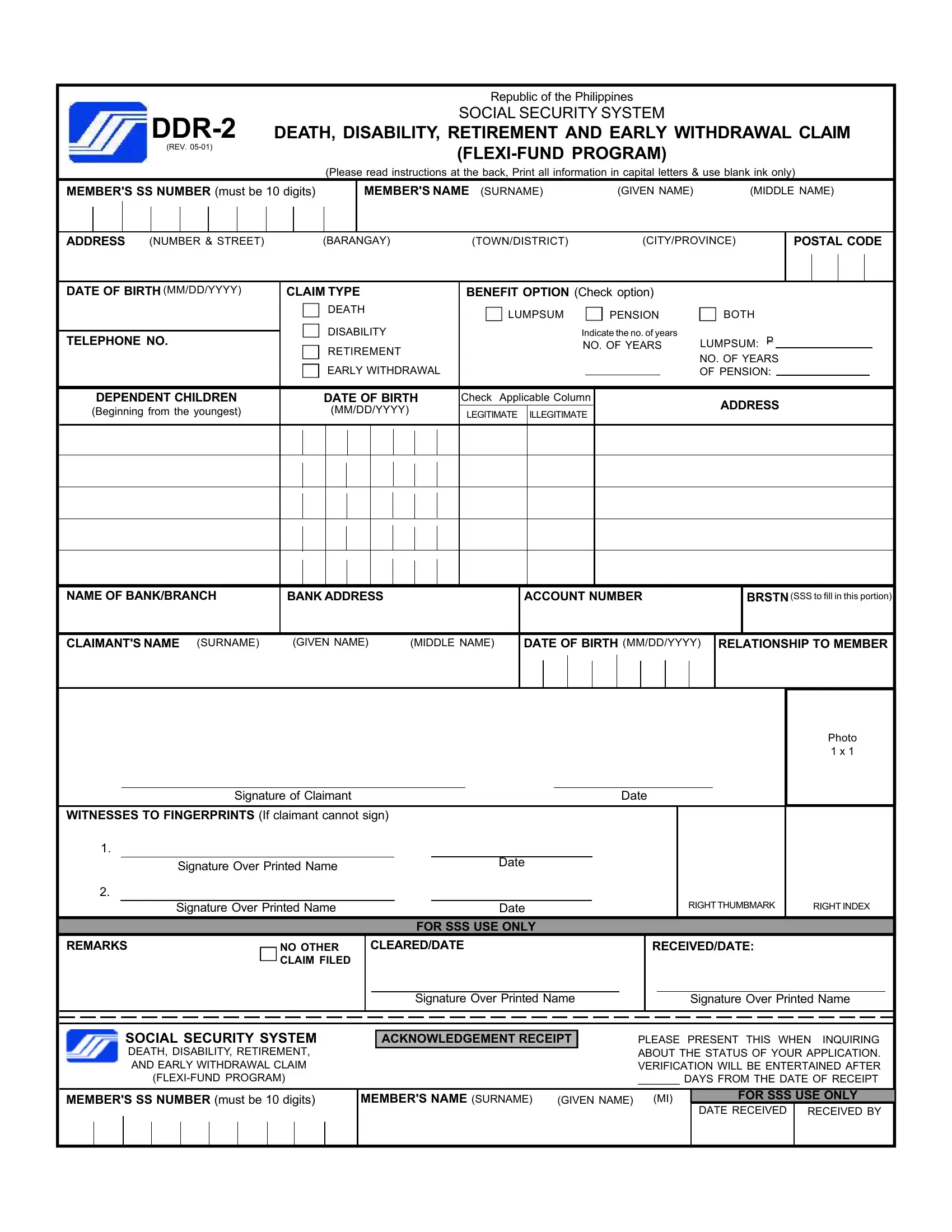
- SS Number: Enter your 10-digit SS number in the numbered boxes at the top. Do not leave any box blank or add dashes between digits.
- Personal information: Write your last name, first name, and middle name in capital letters. Use the exact name registered with the SSS.
- Address: Provide your current mailing address, including barangay, city or municipality, and province.
- Claim type: Mark the appropriate box: Death, Disability, Retirement, or Early Withdrawal under the Flexi-Fund. Select only one claim type per submission.
- Benefit option: For death and disability claims, choose between a lump-sum payment or a monthly pension. Eligibility rules apply. Retirement and early withdrawal claims follow separate benefit schedules.
- Dependent children: List all unmarried children under 21 years old, including full names and dates of birth. Permanently disabled children may be listed without an age limit.
- Banking details: Enter your bank name, branch, and savings account number. The SSS disburses all payments directly to the account provided.
- Declaration: Sign and date the declaration to certify that all information is true and correct. False declarations carry criminal liability under Philippine law.
Required Documents by Claim Type
Prepare documents before visiting the SSS branch. Incomplete submissions are returned and delay processing.
- Death benefit claim: Original death certificate, birth certificate or marriage certificate of the beneficiary, 2 valid government-issued photo IDs
- Disability claim: Certificate from an SSS-accredited physician, hospital records or accident reports, employer certification if applicable
- Retirement claim: Original PSA-certified birth certificate, proof of cessation of employment, 2 valid IDs
- Early Flexi-Fund withdrawal: Flexi-Fund passbook or account statement, 2 valid government IDs, updated membership data form if records need correction
Where to Submit
Submit the completed form with all required documents to your nearest SSS branch. Processing takes 30 to 60 days after the SSS receives a complete submission. Track your claim status through the My.SSS member portal online.
Related SSS Forms
Confirm your member data is current before filing. Use the E4 Form SSS to update your registered personal information. Employers verifying contribution records may need the SSS Contribution R-3 Form. Members filing a disability claim may also need a separate disability claim form completed by their attending physician.