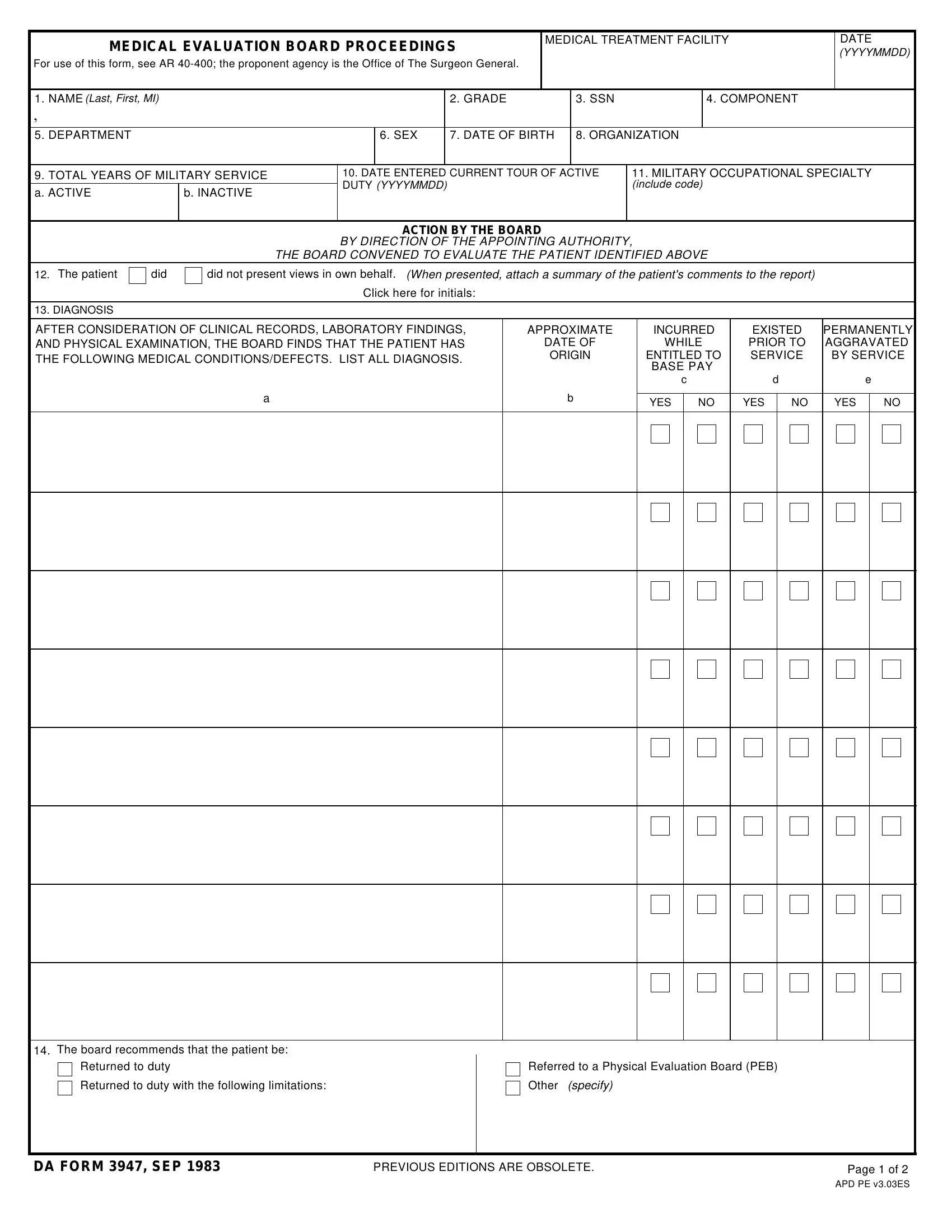
The DA 3947 form is also known as the Medical Evaluation Board Proceedings. It plays a vital role for military personnel facing medical challenges. The form is governed by AR 40-400 and overseen by the Office of The Surgeon General.
This document provides a complete record of the medical evaluation process. It captures personal identification data such as name, grade, and service number. It also documents military service history, covering both active and inactive service periods.
The board uses the form to record its findings after reviewing clinical records, laboratory results, and physical examinations. Each medical condition or defect is listed with a diagnosis. The form notes whether the condition originated prior to service or was aggravated by service.
Based on the findings, the board recommends one of several actions. These include a return to duty, assignment with limitations, or referral to a Physical Evaluation Board. The form also captures whether the service member presented personal views during the proceedings.
The approving authority records its final decision on the form. Service members can file an appeal if they disagree with the board's determination. The DA 3947 is a critical tool in protecting the health and career welfare of each service member.
| Question | Answer |
|---|---|
| Form Name | Da 3947 Form |
| Form Length | 3 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 45 sec |
| Other names | da3947, narsum example, da form 3947 pdf fillable, da 3947 |