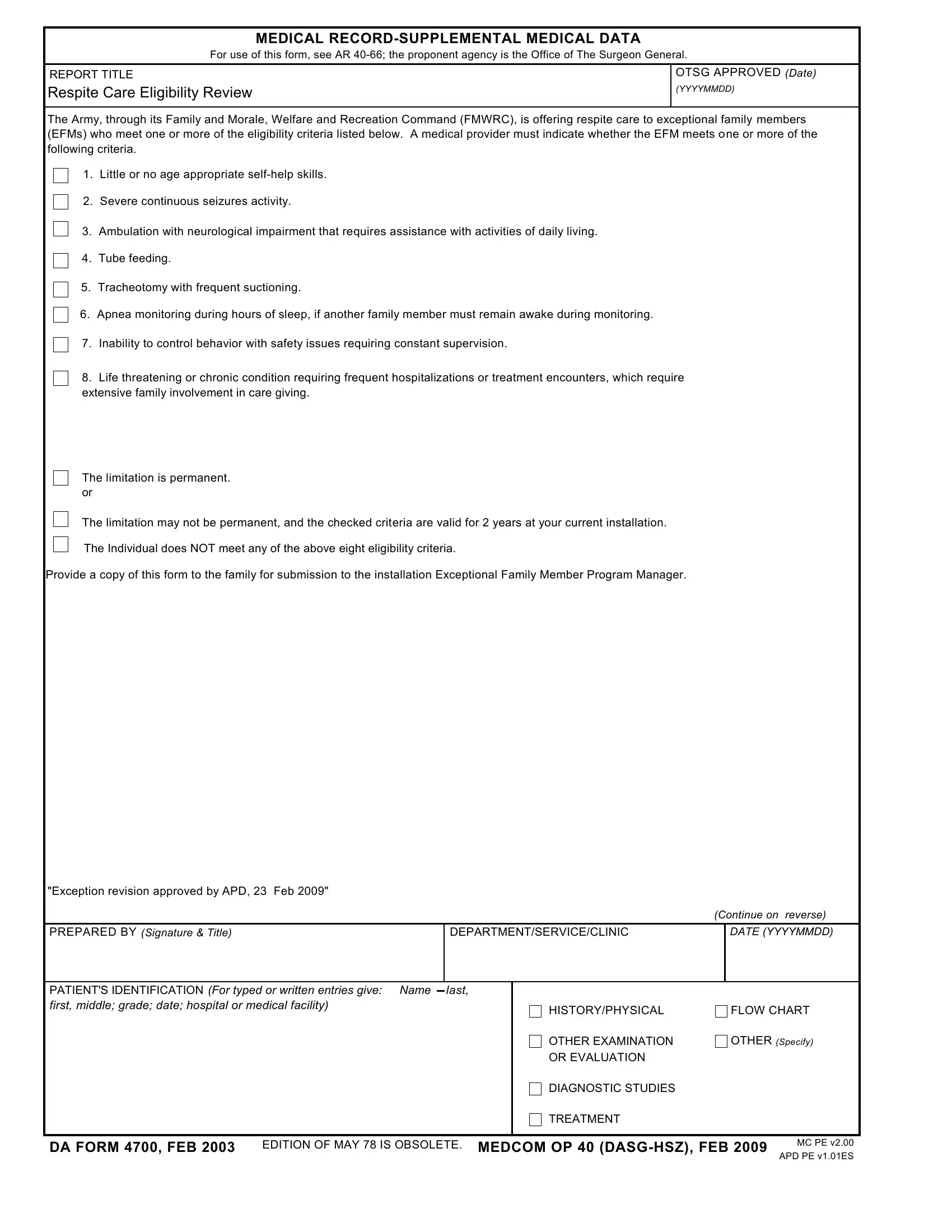
Understanding the intricacies of military family support is crucial, especially when it pertains to the health care and welfare of exceptional family members (EFMs). The DA Form 4700 serves as a vital tool in this regard, designed to document supplemental medical data important for evaluating eligibility for respite care under the Family and Morale, Welfare and Recreation Command (FMWRC). The form requires a detailed medical provider's assessment to determine if an EFM meets specific criteria, such as lacking age-appropriate self-help skills, experiencing severe continuous seizure activity, or requiring constant supervision due to safety issues, among others. This assessment not only identifies those in need of additional support due to severe health conditions but also outlines the type of care required, whether it involves assistance with daily living activities due to neurological impairment, tube feeding, tracheotomy care, apnea monitoring, or frequent hospitalizations. With eligibility criteria clearly listed and a process in place for review every two years—or at the next duty station—the DA Form 4700 embodies a structured approach to providing necessary relief and support to military families, ensuring their exceptional members' needs are adequately recognized and met. The form also underscores the importance of continuity of care, requiring the family to submit a copy to the installation Exceptional Family Member Program Manager, thereby fostering a collaborative effort to maintain the well-being of EFMs.
| Question | Answer |
|---|---|
| Form Name | Da 4700 Form |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | da form 4700 pdf, dd 4700, da form 4700, dd form 4700 |
MEDICAL
For use of this form, see AR
REPORT TITLE
Respite Care Eligibility Review
OTSG APPROVED (Date)
(YYYYMMDD)
The Army, through its Family and Morale, Welfare and Recreation Command (FMWRC), is offering respite care to exceptional family members (EFMs) who meet one or more of the eligibility criteria listed below. A medical provider must indicate whether the EFM meets one or more of the following criteria.
1. Little or no age appropriate
2. Severe continuous seizures activity.
3. Ambulation with neurological impairment that requires assistance with activities of daily living.
4. Tube feeding.
5. Tracheotomy with frequent suctioning.
6. Apnea monitoring during hours of sleep, if another family member must remain awake during monitoring.
7. Inability to control behavior with safety issues requiring constant supervision.
8. Life threatening or chronic condition requiring frequent hospitalizations or treatment encounters, which require extensive family involvement in care giving.
The limitation is permanent. or
The limitation may not be permanent, and the checked criteria are valid for 2 years at your current installation.
The Individual does NOT meet any of the above eight eligibility criteria.
Provide a copy of this form to the family for submission to the installation Exceptional Family Member Program Manager.
"Exception revision approved by APD, 23 Feb 2009"
|
|
(Continue on reverse) |
|
|
|
|
|
PREPARED BY (Signature & Title) |
DEPARTMENT/SERVICE/CLINIC |
|
DATE (YYYYMMDD) |
|
|
|
|
PATIENT'S IDENTIFICATION (For typed or written entries give: Name |
|
last, |
|
|
|
|
|
||
first, middle; grade; date; hospital or medical facility) |
HISTORY/PHYSICAL |
FLOW CHART |
||
|
|
|
||
|
|
|
OTHER EXAMINATION |
OTHER (Specify) |
|
|
|
OR EVALUATION |
|
|
|
|
DIAGNOSTIC STUDIES |
|
|
|
|
TREATMENT |
|
DA FORM 4700, FEB 2003 EDITION OF MAY 78 IS OBSOLETE. MEDCOM OP 40
MC PE v2.00
APD PE v1.01ES