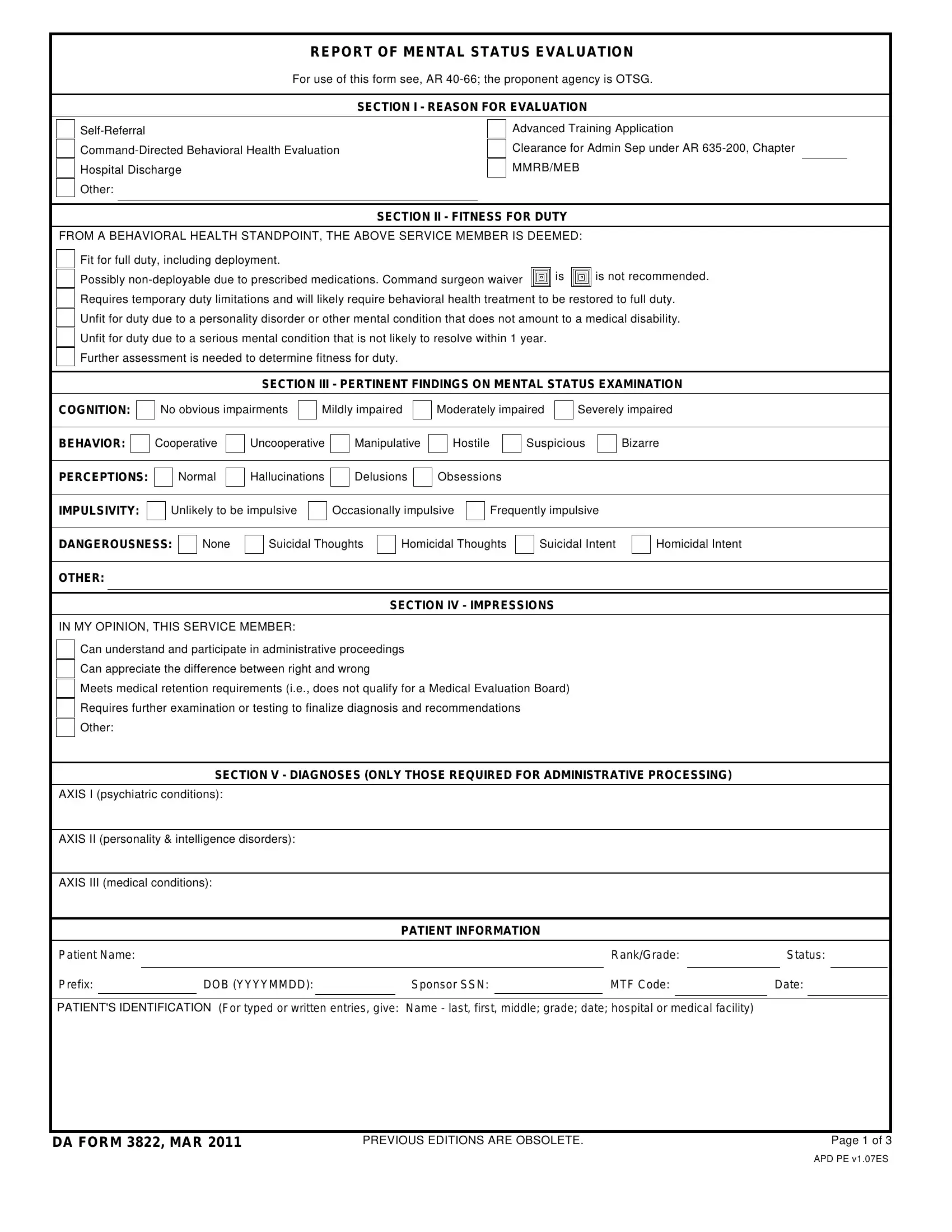
In the evolving landscape of military health and well-being, the DA Form 3822, titled "Report of Mental Status Evaluation," plays a crucial role. At its core, the document is structured to assess a service member's mental fitness for duty, addressing a range of considerations from deployability to the need for medical or behavioral health interventions. The detailed form serves multiple purposes, starting with clarifying the reason for evaluation, which can stem from self-referral, command-directed assessment, or other sources such as hospital discharge or the necessity for administrative separation under specific regulations. Evaluators use this form to document a wide spectrum of mental health statuses, assessing fitness for duty with a nuanced approach that may include temporary limitations, potential non-deployability due to medication, or assessing the severity of mental conditions that impact duty readiness. Pertinent findings in areas such as cognition, behavior, perceptions, and impulsivity provide a structured overview that informs subsequent decisions. Moreover, it encompasses recommendations for treatment, precautionary measures to ensure safety, and final impressions that guide administrative actions. This comprehensive evaluation process illustrates an effort to balance operational readiness with the nuanced understanding of behavioral health, signifying the military's recognition of the complexity of mental health issues and their potential impact on service members' capabilities and overall unit effectiveness.
| Question | Answer |
|---|---|
| Form Name | Da Form 3822 |
| Form Length | 3 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 45 sec |
| Other names | da 3822 pdf, da form 3822, da form 3822 june 2019, da 3822 fillable |
REPORT OF MENTAL STATUS EVALUATION
For use of this form see, AR
SECTION I - REASON FOR EVALUATION
Other:
Advanced Training Application
Clearance for Admin Sep under AR
MMRB/MEB
SECTION II - FITNESS FOR DUTY
FROM A BEHAVIORAL HEALTH STANDPOINT, THE ABOVE SERVICE MEMBER IS DEEMED: |
|
|||
Fit for full duty, including deployment. |
|
|
|
|
Possibly |
|
is |
|
is not recommended. |
|
|
|
|
|
|
|
|
|
|
Requires temporary duty limitations and will likely require behavioral health treatment to be restored to full duty. |
||||
Unfit for duty due to a personality disorder or other mental condition that does not amount to a medical disability. |
||||
Unfit for duty due to a serious mental condition that is not likely to resolve within 1 year. |
|
|
|
|
Further assessment is needed to determine fitness for duty. |
|
|
|
|
SECTION III - PERTINENT FINDINGS ON MENTAL STATUS EXAMINATION
COGNITION:
No obvious impairments
Mildly impaired
Moderately impaired
Severely impaired
BEHAVIOR:
Cooperative
Uncooperative
Manipulative
Hostile
Suspicious
Bizarre
PERCEPTIONS:
Normal
Hallucinations
Delusions
Obsessions
IMPULSIVITY:
Unlikely to be impulsive
Occasionally impulsive
Frequently impulsive
DANGEROUSNESS:
None
Suicidal Thoughts
Homicidal Thoughts
Suicidal Intent
Homicidal Intent
OTHER:
SECTION IV - IMPRESSIONS
IN MY OPINION, THIS SERVICE MEMBER:
Can understand and participate in administrative proceedings
Can appreciate the difference between right and wrong
Meets medical retention requirements (i.e., does not qualify for a Medical Evaluation Board)
Requires further examination or testing to finalize diagnosis and recommendations
Other:
SECTION V - DIAGNOSES (ONLY THOSE REQUIRED FOR ADMINISTRATIVE PROCESSING)
AXIS I (psychiatric conditions):
AXIS II (personality & intelligence disorders):
AXIS III (medical conditions):
PATIENT INFORMATION
Patient Name: |
|
|
|
|
Rank/Grade: |
|
Status: |
||||||
|
|
|
|
|
|
|
|
|
|
|
|
||
Prefix: |
|
DOB (YYYYMMDD): |
|
Sponsor SSN: |
|
MTF Code: |
|
Date: |
|
||||
PATIENT'S IDENTIFICATION (For typed or written entries, give: Name - last, first, middle; grade; date; hospital or medical facility)
DA FORM 3822, MAR 2011 |
PREVIOUS EDITIONS ARE OBSOLETE. |
Page 1 of 3 |
APD PE v1.07ES
SECTION VI - PROPOSED TREATMENTS
None
Clinic: |
Phone No: |
Location: |
Date: |
Time: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Recommend command referral to:
Unit Chaplain
ASAP
FAP
JAG
ACS
OTHER
SECTION VII - RECOMMENDED PRECAUTIONS
(To be followed until no longer deemed necessary by a Behavior Heath Provider)
None. |
|
|
|
|
|
|
Ensure the service member attends all |
|
|
||||
Assigned duties should be relatively |
|
should not involve leadership responsibilities. |
||||
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Work hours should not exceed |
|
per day and the service member should have |
|
day(s) off per week. |
||
|
|
|
|
|
|
|
Restrict access to or disarm all weapons and ammunition (including those that are privately owned).
Prohibit the use of alcohol as alcohol is a CNS depressant and may impair inhibitions and judgment,
Inspect the service member's quarters and secure all hazardous items (e.g., pills, knives, razors, weapons, etc.).
Move the service member into the barracks.
Secure all medications and dispense no more than |
days' worth at a time. |
|||||
|
|
|
|
|
|
|
Prohibit contact between the service member and |
|
|
to prevent harm to self or other individual. |
|||
|
|
|
|
|
||
Provide increased supervision (i.e., have someone check in with service member at least daily) or ... |
||||||
Assign someone to monitor the service member every |
|
hours from first formation until lights out, and |
||||
|
|
|
|
|
||
ensure he/she does not sleep in a room alone or ... |
|
|
|
|||
Provide continuous 24/7 monitoring (e.g., to prevent
Other:
SECTION VIII - ADDITIONAL COMMENTS
|
|
A Temporary Profile with an "S" rating of |
|
|
|
|
is hereby activated, to expire |
|
|
|
|
|
|
|
|
|
|
. |
|
|
|
|
|
|
||||||||||||||||||||
|
|
The service member has been screened for Post Traumatic Stress Disorder and mild Traumatic Brain Injury. All positive screens require a |
||||||||||||||||||||||||||||||||||||||||||
|
|
|||||||||||||||||||||||||||||||||||||||||||
|
|
comprehensive evaluation. Results of the screening are as follows: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||
|
|
|
|
|
Post Traumatic Stress Disorder Screening: |
|
|
Score |
|
|
|
|
|
Positive |
|
|
Negative |
|
|
|
|
|
|
|
||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Service member was referred for: A comprehensive Post Traumatic Stress Disorder evaluation. |
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Mild Traumatic Brain Injury Screening: |
|
|
Score |
|
|
|
Positive |
|
Negative |
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||
|
|
|
|
|
|
|
|
Service member was referred for: A comprehensive mild Traumatic Brain Injury evaluation. |
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
The service member may participate in PT as allowed by physical profile, as exercise often improves mood. |
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||||||
|
|
The service member meets psychiatric criteria for expeditious administrative separation lAW |
|
Chapter |
|
|
Chapter |
|||||||||||||||||||||||||||||||||||||
|
|
|
|
|
||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
||||||||||||||||||||||||||||||||||||||||
|
|
(or equivalent regulation from his/her branch of Service). |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
(See Additional Comments on Page 3) |
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PATIENT INFORMATION |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
Patient Name: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Rank/Grade: |
|
|
|
Status: |
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
Prefix: |
|
|
|
|
|
DOB (YYYYMMDD): |
|
|
|
|
|
|
|
Sponsor SSN: |
|
|
|
|
|
|
|
MTF Code: |
|
|
|
Date: |
|
|
|||||||||||||||
PATIENT'S IDENTIFICATION (For typed or written entries, give: Name - last, first, middle; grade; date; hospital or medical facility)
DA FORM 3822, MAR 2011 |
Page 2 of 3 |
APD PE v1.07ES
SECTION VIII - ADDITIONAL COMMENTS (Continued from previous page)
Service member does not have a severe mental disorder and is not considered mentally disordered. However, he/she has a
The
It is the professional opinion of the undersigned that this service member will not respond to command efforts at rehabilitation (such as transfer, disciplinary action or reclassification), or to any behavioral health treatment methods currently available in the military.
The service member manifests a
The service member shows no evidence of a disorder that would limit his/her potential to succeed in the military. He/she is cleared to participate in advanced military training.
The service member has been screened for Post Traumatic Stress Disorder and Traumatic Brain Injury. These conditions are either not present or, if present, do not meet AR
If the service member shows signs of further deterioration, command should call: Name: |
|
and Contact |
||
Information: |
, during duty hours. After hours, they should escort the service member to the nearest |
|||
|
|
|
|
|
Emergency Department. |
|
|
|
|
Service member has been screened for substance use disorders (i.e., alcohol and drugs).
Findings:
Other:
|
|
|
|
|
|
|
REMARKS |
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
BEHAVIORAL HEALTH PROVIDER SIGNATURE(S) |
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Behavioral Health Provider's Signature |
|
Date |
|
Behavioral Health Supervisory |
|
|
Date |
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PATIENT INFORMATION |
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
Patient Name: |
|
|
|
|
|
|
|
|
Rank/Grade: |
|
Status: |
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
Prefix: |
|
DOB (YYYYMMDD): |
|
|
|
Sponsor SSN: |
|
MTF Code: |
|
Date: |
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|||||||||
PATIENT'S IDENTIFICATION (For typed or written entries, give: |
Name - last, first, middle; grade; date; hospital or medical facility) |
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
DA FORM 3822, MAR 2011 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Page 3 of 3 |
||||
APD PE v1.07ES