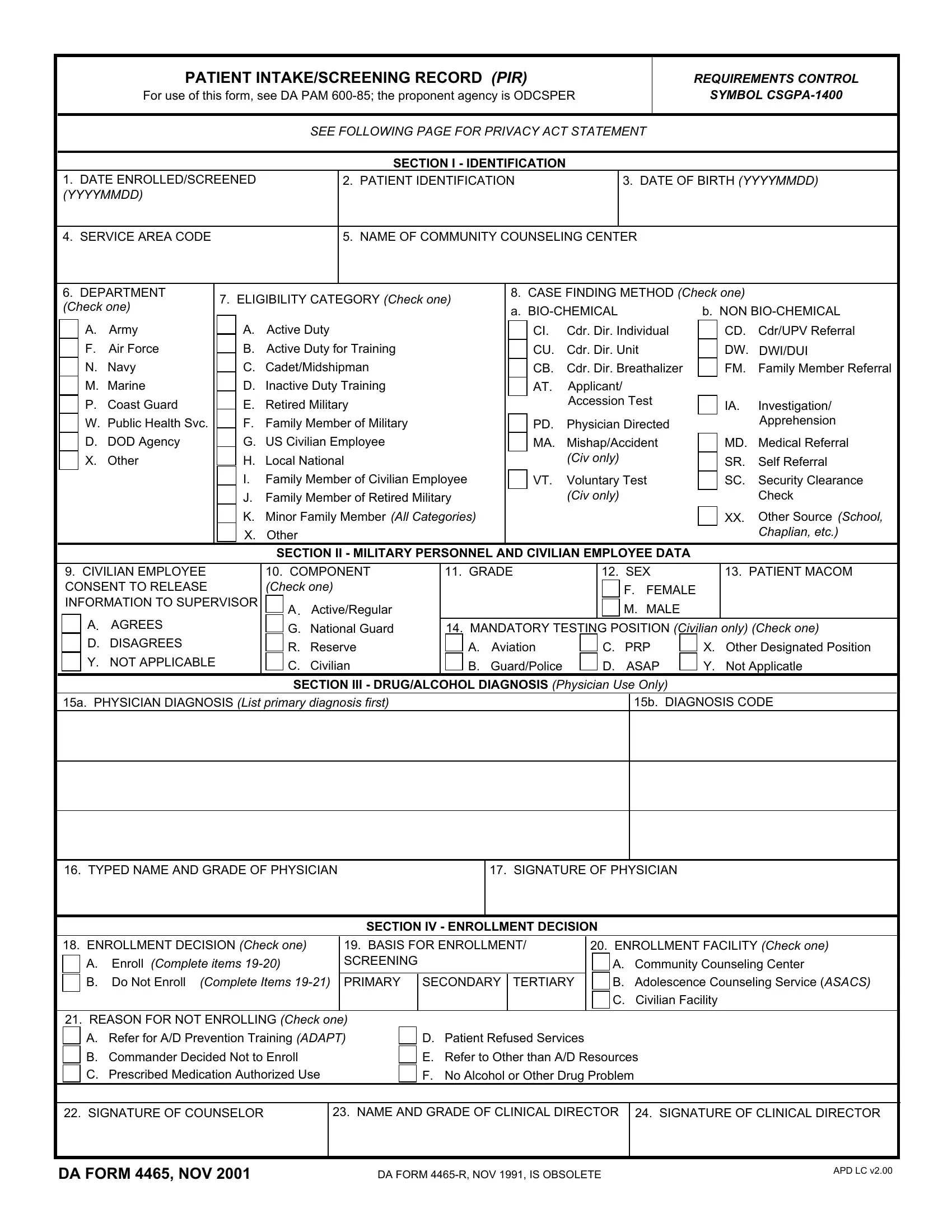
The DA 4465 form, officially known as the Patient Intake/Screening Record (PIR), plays a crucial role in the administrative framework of the Department of Defense, particularly within the context of the Army Substance Abuse Program (ASAP). This form is designed to facilitate the intake and screening processes for individuals seeking support for substance-related concerns, ensuring that detailed information about the patient's identity, military or civilian employment status, and diagnostic findings are meticulously recorded. The process articulated in DA PAM 600-85, with the proponent agency being the Office of the Deputy Chief of Staff for Personnel (ODCSPER), underscores the significance of systematic documentation in delivering comprehensive care and support. The form encompasses various sections that collect essential information ranging from basic identification details, eligibility categories, case finding methods to military personnel or civilian employee data, thereby offering a structured approach to patient intake. By highlighting the mechanisms for enrollment decisions and the confidentiality embraced through the Privacy Act Statement, the DA 4465 form serves as a pivotal tool in the operationalization of the ASAP, aiming to balance the demand for service member accountability with the imperative of providing empathetic care and rehabilitation services. With its mandatory disclosure for active duty members and the implications of non-compliance for civilian employees, the form encapsulates a blend of procedural rigidity and the commitment to health and recovery within the military community.
| Question | Answer |
|---|---|
| Form Name | Da Form 4465 |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | patient screening record pir, patient pir form, pir armypubs fillable, da 4465 form |
PATIENT INTAKE/SCREENING RECORD (PIR)
For use of this form, see DA PAM
REQUIREMENTS CONTROL
SYMBOL
SEE FOLLOWING PAGE FOR PRIVACY ACT STATEMENT
SECTION I - IDENTIFICATION
|
|
1. DATE ENROLLED/SCREENED |
|
|
2. PATIENT IDENTIFICATION |
|
|
|
3. DATE OF BIRTH (YYYYMMDD) |
|||||||||||||||||
|
|
(YYYYMMDD) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
4. SERVICE AREA CODE |
|
|
|
|
5. NAME OF COMMUNITY COUNSELING CENTER |
|
|
|
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
6. DEPARTMENT |
|
7. ELIGIBILITY CATEGORY (Check one) |
|
|
8. CASE FINDING METHOD (Check one) |
|
|
|||||||||||||||||
|
|
(Check one) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
a. |
|
|
b. NON |
||||||||||||
|
|
|
|
A. |
Army |
|
|
A. |
Active Duty |
|
|
|
|
CI. |
Cdr. Dir. Individual |
|
|
CD. |
Cdr/UPV Referral |
|||||||
|
|
|
|
|
|
|||||||||||||||||||||
|
|
|
|
F. |
Air Force |
|
|
B. |
Active Duty for Training |
|
|
|
|
CU. |
Cdr. Dir. Unit |
|
|
DW. |
DWI/DUI |
|||||||
|
|
|
|
|
|
|||||||||||||||||||||
|
|
|
|
N. |
Navy |
|
|
C. |
Cadet/Midshipman |
|
|
|
|
CB. |
Cdr. Dir. Breathalizer |
|
|
FM. |
Family Member Referral |
|||||||
|
|
|
|
|
|
|||||||||||||||||||||
|
|
|
|
M. Marine |
|
|
D. |
Inactive Duty Training |
|
|
|
|
AT. |
Applicant/ |
|
|
|
|
|
|
|
|||||
|
|
|
|
P. |
Coast Guard |
|
|
E. |
Retired Military |
|
|
|
|
|
Accession Test |
|
|
IA. |
Investigation/ |
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
W. |
Public Health Svc. |
|
|
F. |
Family Member of Military |
|
|
|
|
PD. |
Physician Directed |
|
|
|
Apprehension |
|||||||
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||
|
|
|
|
D. |
DOD Agency |
|
|
G. |
US Civilian Employee |
|
|
|
|
MA. |
Mishap/Accident |
|
|
MD. |
Medical Referral |
|||||||
|
|
|
|
|
|
|||||||||||||||||||||
|
|
|
|
X. |
Other |
|
|
H. |
Local National |
|
|
|
|
|
(Civ only) |
|
|
|
|
SR. |
Self Referral |
|||||
|
|
|
|
|
|
|
|
I. |
Family Member of Civilian Employee |
|
|
|
VT. |
Voluntary Test |
|
|
SC. |
Security Clearance |
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
|
|
|
|
|
|
|
|
J. |
Family Member of Retired Military |
|
|
|
|
(Civ only) |
|
|
|
|
|
Check |
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
K. |
Minor Family Member (All Categories) |
|
|
|
|
|
|
|
|
|
|
|
XX. |
Other Source (School, |
||||
|
|
|
|
|
|
|
|
X. |
Other |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Chaplian, etc.) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
SECTION II - MILITARY PERSONNEL AND CIVILIAN EMPLOYEE DATA |
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
|
9. CIVILIAN EMPLOYEE |
|
|
10. COMPONENT |
11. GRADE |
|
12. SEX |
|
|
13. PATIENT MACOM |
|||||||||||||||
|
|
CONSENT TO RELEASE |
|
|
(Check one) |
|
|
|
|
|
|
|
|
F. FEMALE |
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
INFORMATION TO SUPERVISOR |
A. |
Active/Regular |
|
|
|
|
|
|
|
|
M. MALE |
|
|
|
|
|
||||||||
|
|
|
|
A. |
AGREES |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
G. National Guard |
14. MANDATORY TESTING POSITION (Civilian only) (Check one) |
|||||||||||||||||||
|
|
|
|
D. DISAGREES |
|
|
R. |
Reserve |
A. |
Aviation |
|
C. |
PRP |
X. |
|
Other Designated Position |
||||||||||
|
|
|
|
Y. NOT APPLICABLE |
|
|
C. |
Civilian |
B. |
Guard/Police |
|
D. |
ASAP |
Y. |
|
Not Applicatle |
||||||||||
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
SECTION III - DRUG/ALCOHOL DIAGNOSIS (Physician Use Only) |
|
|
|
|
|
||||||||||||
|
|
15a. PHYSICIAN DIAGNOSIS (List primary diagnosis first) |
|
|
|
|
|
|
|
|
|
15b. DIAGNOSIS CODE |
||||||||||||||
16. TYPED NAME AND GRADE OF PHYSICIAN
17. SIGNATURE OF PHYSICIAN
SECTION IV - ENROLLMENT DECISION
18. ENROLLMENT DECISION (Check one) |
19. BASIS FOR ENROLLMENT/ |
20. ENROLLMENT FACILITY (Check one) |
||||
A. |
Enroll (Complete items |
SCREENING |
|
|
A. |
Community Counseling Center |
B. |
Do Not Enroll (Complete Items |
PRIMARY |
SECONDARY |
TERTIARY |
B. |
Adolescence Counseling Service (ASACS) |
|
|
|
|
|
C. |
Civilian Facility |
|
|
|
|
|
|
|
21. REASON FOR NOT ENROLLING (Check one) |
|
|
|
|
||
A. Refer for A/D Prevention Training (ADAPT) |
D. Patient Refused Services |
|
|
|||
B. Commander Decided Not to Enroll |
|
E. Refer to Other than A/D Resources |
||||
C. |
Prescribed Medication Authorized Use |
|
F. No Alcohol or Other Drug Problem |
|
||
22. SIGNATURE OF COUNSELOR
23. NAME AND GRADE OF CLINICAL DIRECTOR
24. SIGNATURE OF CLINICAL DIRECTOR
DA FORM 4465, NOV 2001 |
DA FORM |
APD LC v2.00 |
|
PRIVACY ACT STATEMENT
AUTHORITY: 5 USC Section 301, Department Regulations; 10 USC Section 3013, Secretary of the Army; 42 USC Section 290dd; Army Regulation
PRINCIPAL PURPOSE: Information is used to treat, counsel, and rehabilitate individuals who participate in the ASAP.
ROUTINE USES: The Patient Administration Division at the medical treatment facility with jurisdicion is responsible for the release of medical information to malpractice insurers in event of malpractice litigation or prospect thereof. Information is disclosed only to the following persons/agencies: to health care components of the Department of Veterans Affairs furnishing health care to veterans; to medical personnel to the extent necessary to meet a bonafide medical emergency; to qualified personnel conducting scientific research, audits or program evaluations, provided that a patient may not be identified in such reports, or his or her identify further disclosed by such personnel; upon the order of a court of competent jurisdiction.
DISCLOSURE: Mandatory for active duty service members. Failure to provide required information may be subject to appropriate disciplinary action under the UCMJ. Voluntary for civilian employees. However, failure to provide all the requested information will prohibit processing comprehensive treatment.
DA FORM 4465, NOV 2001 |
Page 2 of 2 |
APD LC v2.00