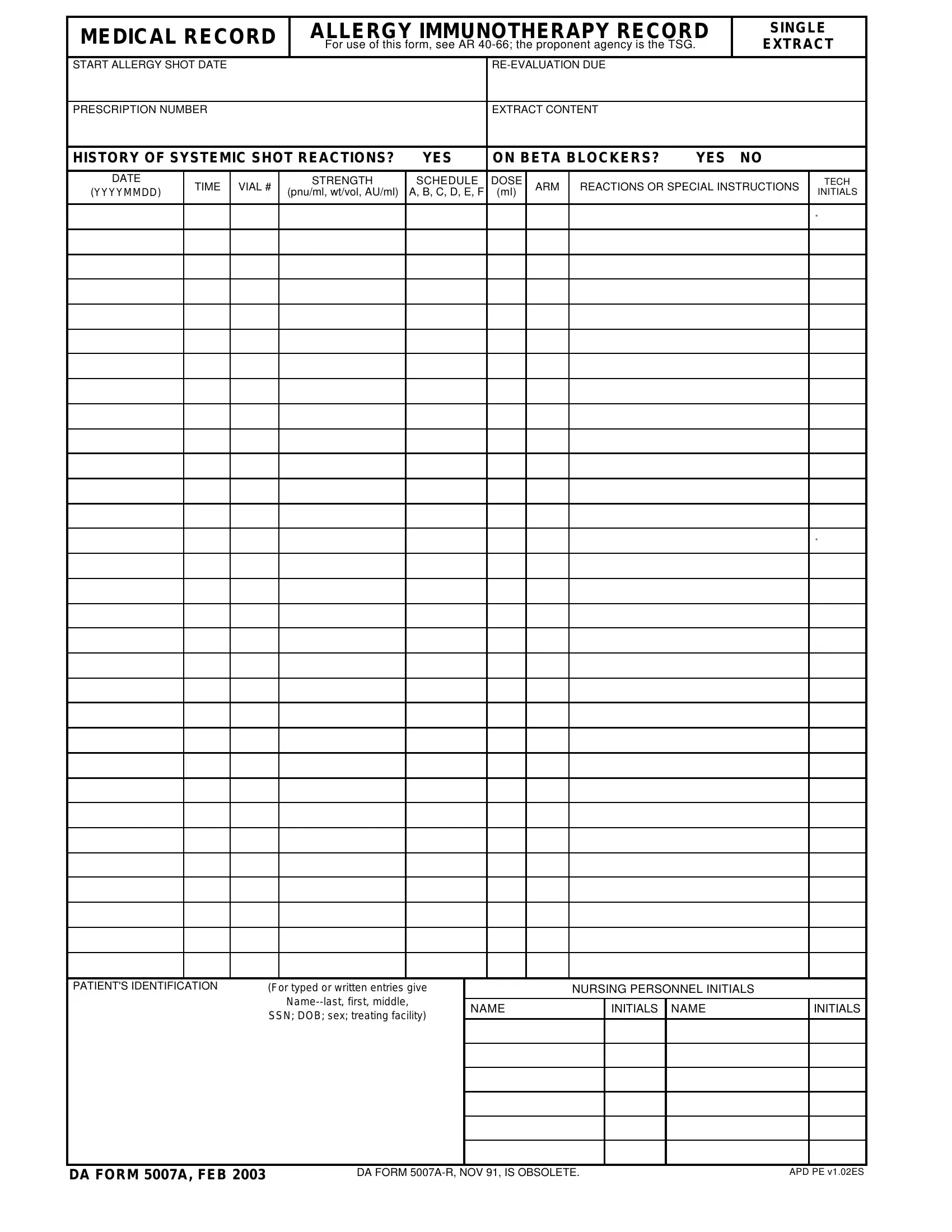
Military members are required to complete a variety of forms, and the Da Form 5007A is one such form. This form is used to record information about a soldier's military occupational specialty (MOS). The information on this form can be helpful for soldiers both currently in the military and those who have left the military. Completing this form correctly is important, so it's important to understand what's required. In this blog post, we'll go over the specifics of the Da Form 5007A. We'll also provide some tips on how to complete it correctly. Let's get started!
| Question | Answer |
|---|---|
| Form Name | Da Form 5007A |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | 2003, 5007A, YYYYMMDD, v1 |
MEDICAL RECORD |
|
ALLERGY IMMUNOTHERAPY RECORD |
SINGLE |
||||||||||||
|
For use of this form, see AR |
EXTRACT |
|||||||||||||
START ALLERGY SHOT DATE |
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
||||
PRESCRIPTION NUMBER |
|
|
|
|
|
|
EXTRACT CONTENT |
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|||||||
HISTORY OF SYSTEMIC SHOT REACTIONS? |
YES |
|
ON BETA BLOCKERS? |
YES |
NO |
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
DATE |
TIME |
VIAL # |
|
STRENGTH |
|
SCHEDULE |
DOSE |
ARM |
REACTIONS OR SPECIAL INSTRUCTIONS |
TECH |
|||||
(YYYYMMDD) |
(pnu/ml, wt/vol, AU/ml) |
|
A, B, C, D, E, F |
(ml) |
INITIALS |
||||||||||
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PATIENT'S IDENTIFICATION |
(For typed or written entries give |
|
|
|
NURSING PERSONNEL INITIALS |
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
NAME |
|
|
INITIALS |
NAME |
|
INITIALS |
|||||
|
|
SSN; DOB; sex; treating facility) |
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
DA FORM 5007A, FEB 2003
DA FORM |
APD PE v1.02ES |