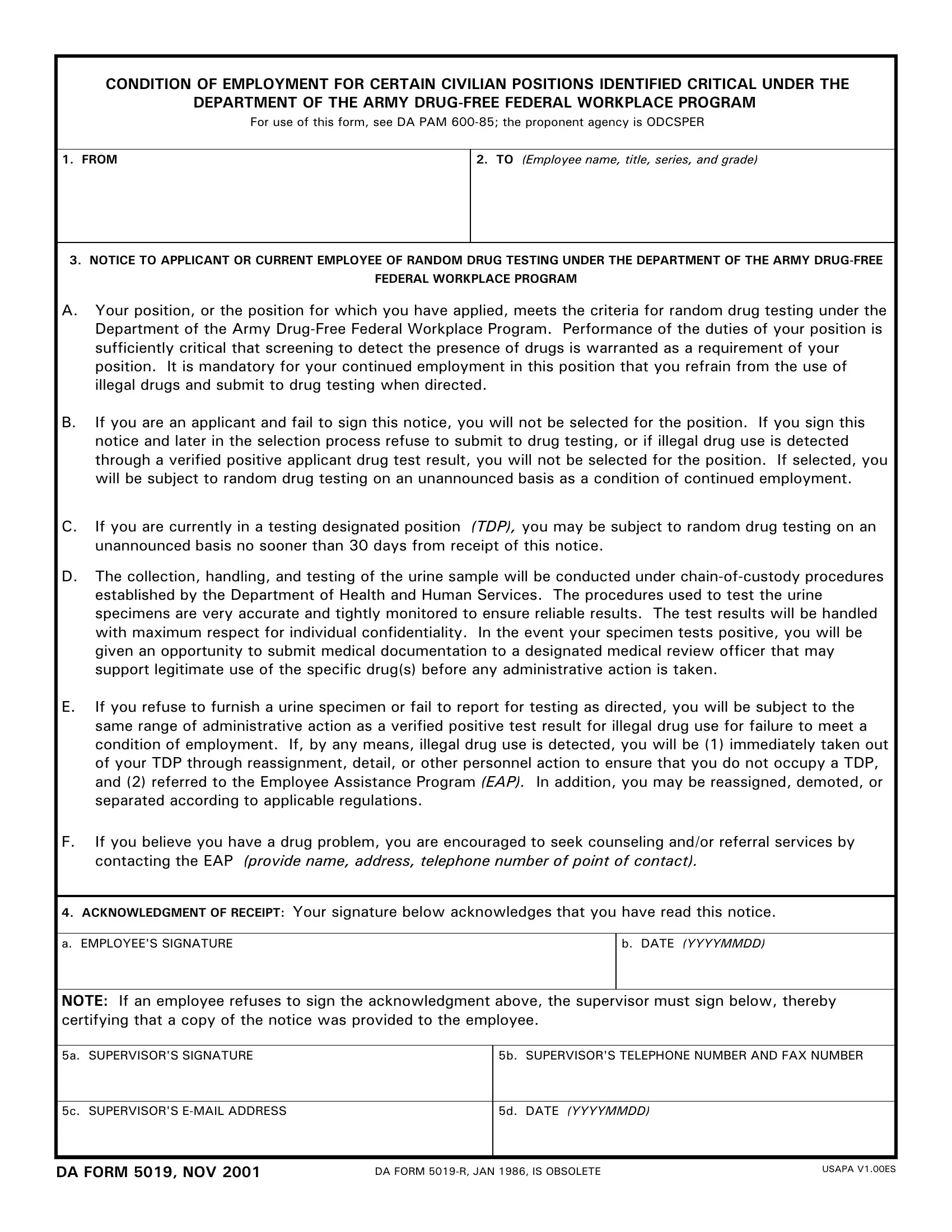
The DA 5019 R form serves a crucial role in maintaining a drug-free environment within the Department of the Army, embodying the stringent measures taken to uphold the standards of a drug-free federal workplace. This form is primarily utilized in notifying applicants or current employees of the necessity for random drug testing as a condition of their employment for positions identified as critical. The essence of this form lies in its comprehensive coverage of the procedures and implications tied to the drug testing program, including mandatory submission to drug testing, the consequences of failing to comply, and the protocols for handling test results with the utmost respect for individual confidentiality. It further outlines the actions that will be taken should an employee fail to meet these conditions, ranging from reassignment to potential separation from employment, and offers guidance on seeking assistance for drug-related issues through the Employee Assistance Program (EAP). By requiring an acknowledgment of receipt from the employee, or a certification by the supervisor if this is refused, the DA 5019 R form encapsulates a strict adherence to policy while ensuring due process and support for individuals facing drug use challenges, thereby reinforcing the commitment of the Department of the Army to a drug-free workplace.
| Question | Answer |
|---|---|
| Form Name | Da Form 5019 R |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | da form 5019 fillable, form da 5019, da5019, da form 5019 |
CONDITION OF EMPLOYMENT FOR CERTAIN CIVILIAN POSITIONS IDENTIFIED CRITICAL UNDER THE DEPARTMENT OF THE ARMY
For use of this form, see DA PAM
1. FROM
2. TO (Employee name, title, series, and grade)
3.NOTICE TO APPLICANT OR CURRENT EMPLOYEE OF RANDOM DRUG TESTING UNDER THE DEPARTMENT OF THE ARMY
A.Your position, or the position for which you have applied, meets the criteria for random drug testing under the Department of the Army
B.If you are an applicant and fail to sign this notice, you will not be selected for the position. If you sign this notice and later in the selection process refuse to submit to drug testing, or if illegal drug use is detected through a verified positive applicant drug test result, you will not be selected for the position. If selected, you will be subject to random drug testing on an unannounced basis as a condition of continued employment.
C.If you are currently in a testing designated position (TDP), you may be subject to random drug testing on an unannounced basis no sooner than 30 days from receipt of this notice.
D.The collection, handling, and testing of the urine sample will be conducted under
E.If you refuse to furnish a urine specimen or fail to report for testing as directed, you will be subject to the same range of administrative action as a verified positive test result for illegal drug use for failure to meet a condition of employment. If, by any means, illegal drug use is detected, you will be (1) immediately taken out of your TDP through reassignment, detail, or other personnel action to ensure that you do not occupy a TDP, and (2) referred to the Employee Assistance Program (EAP). In addition, you may be reassigned, demoted, or separated according to applicable regulations.
F.If you believe you have a drug problem, you are encouraged to seek counseling and/or referral services by contacting the EAP (provide name, address, telephone number of point of contact).
4. ACKNOWLEDGMENT OF RECEIPT: Your signature below acknowledges that you have read this notice.
a. EMPLOYEE'S SIGNATURE
b. DATE (YYYYMMDD)
NOTE: If an employee refuses to sign the acknowledgment above, the supervisor must sign below, thereby certifying that a copy of the notice was provided to the employee.
5a. SUPERVISOR'S SIGNATURE
5b. SUPERVISOR'S TELEPHONE NUMBER AND FAX NUMBER
5c. SUPERVISOR'S
5d. DATE (YYYYMMDD)
DA FORM 5019, NOV 2001 |
DA FORM |
USAPA V1.00ES |
|