
About Da Form 5181 R
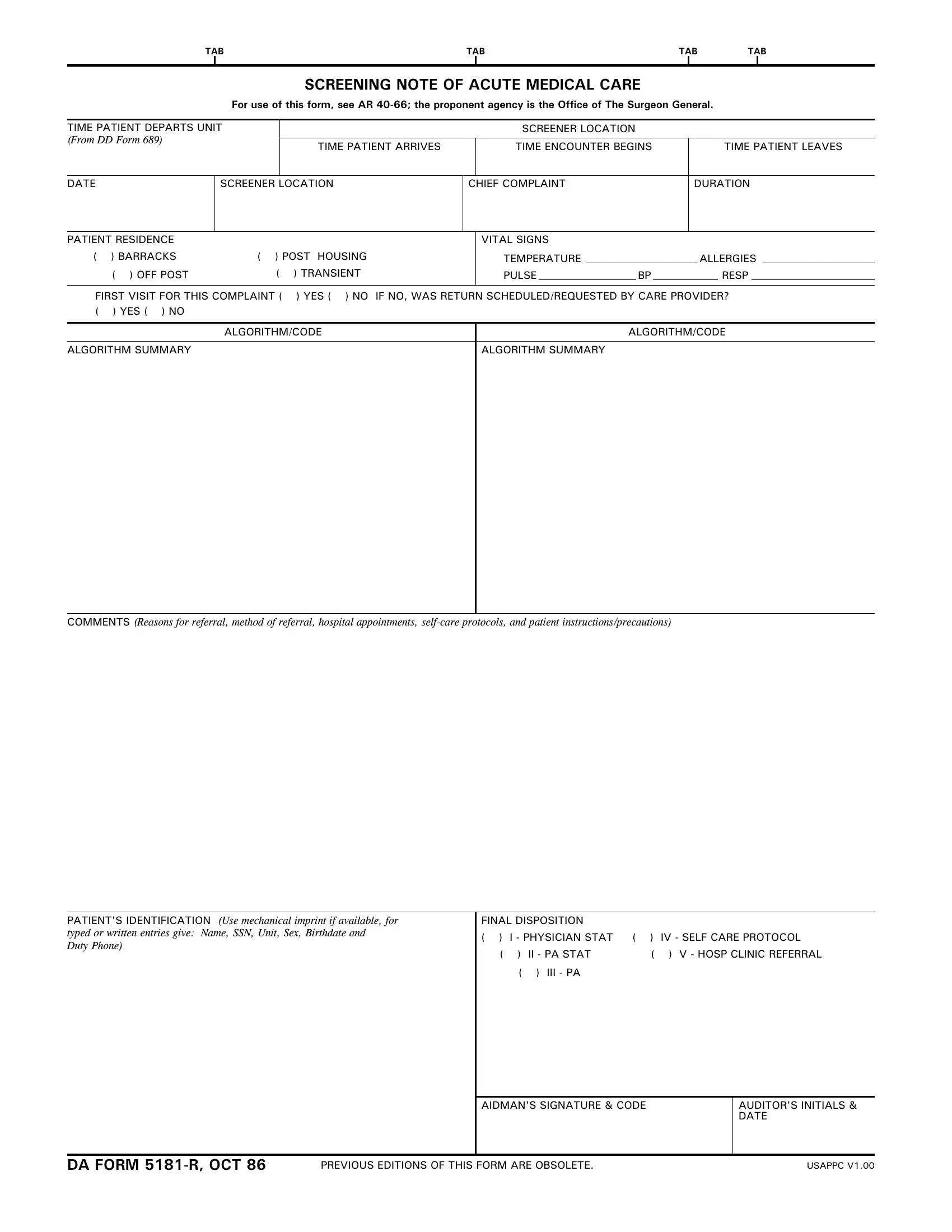
Da Form 5181 R is the Army Screening Note of Acute Medical Care. Military medical providers use this form at the Battalion Aid Station (BAS) level and above to document each acute care visit. It records the full terms of the patient encounter, from departure time and chief complaint through to final care disposition. It is mandatory under AR 40-66 and issued by the Office of The Surgeon General.
Key Fields on the Form
When medical staff fill out this document, they record the following information:
- Patient identification including name, unit, and date of visit
- Time the patient left their unit to seek care
- Vital signs including blood pressure, pulse, temperature, and respirations
- Chief complaint and history of the present illness
- Known allergies to medications or environmental triggers
- Whether the visit is a first contact or a return care appointment
- Final disposition such as return to duty, physician consult, or hospital referral
How to Complete This Medical Care Form
To fill out the document, begin with the patient identification block in Section I. Enter the name, Social Security number, unit, and visit date. Move to Section II to record all vital signs. Describe the chief complaint in clear, plain language. Note any allergy information before indicating treatment. In the final disposition block, record the outcome of the medical care visit and sign the form to close the care record.
How This Form Compares to SF 600
This document acts as an alternative to the SF 600 Health Record at BAS-level facilities. When the patient transfers to a higher care setting, the completed document travels with them. When the patient stays at the BAS, the form remains in the station files. For related military documentation, see the DA Form 4700 and additional Army medical forms.