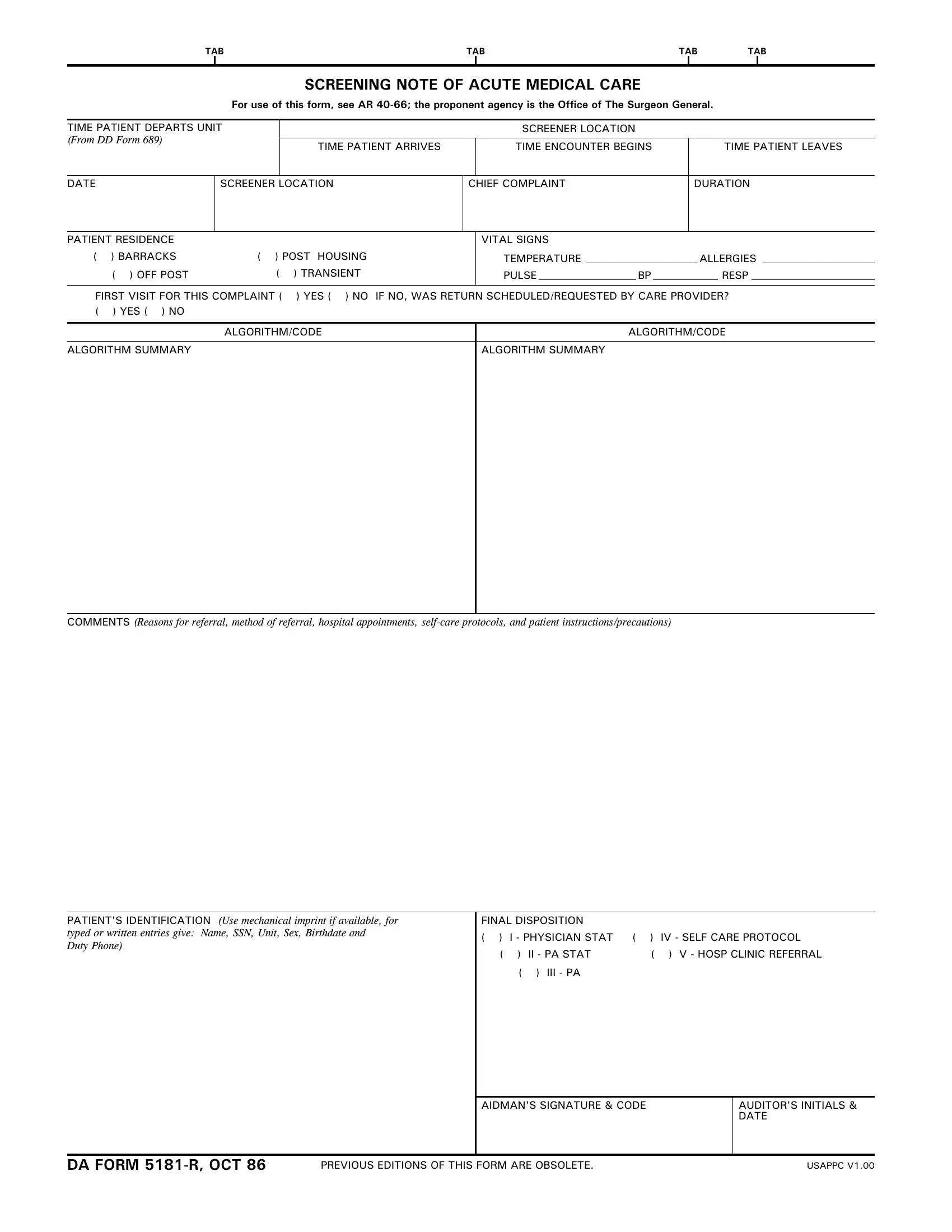
The DA Form 5181 R, known as the Screening Note of Acute Medical Care, plays a crucial role in the documentation and management of medical care within the military context. Mandated by AR 40-66 and developed under the guidance of the Office of The Surgeon General, this form meticulously records various essential aspects of a patient's visit for acute medical care, emphasizing the importance of an accurate and thorough medical documentation process. It captures a series of critical data points—from the time the patient leaves their unit to the final disposition of their visit, including chief complaints, vital signs, residence, and allergy information. This form is not only instrumental in documenting first-time visits but also in tracking follow-up care when necessary, indicating whether a return visit was initiated by the care provider. Furthermore, it encompasses patient identification details and concludes with the final disposition of the patient, which could range from physician consultation to self-care protocols or hospital clinic referrals. The DA Form 5181 R serves as an alternative to the SF 600 (Health Record-Chronological Record of Medical Care) at the Battalion Aid Station (BAS) level and above, ensuring that a comprehensive record accompanies the patient throughout their care journey or remains at the BAS as determined by the patient's disposition. As such, it is an indispensable document for healthcare providers in the military, facilitating not only immediate care decisions but also contributing to the broader healthcare management and audit system.
| Question | Answer |
|---|---|
| Form Name | Da Form 5181 R |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | adtmc army 2019, adtmc app, adtmc 2019, adtmc pdf |
TAB |
TAB |
TAB |
TAB |
||||
|
|
|
|
|
|
|
|
SCREENING NOTE OF ACUTE MEDICAL CARE
For use of this form, see AR
TIME PATIENT DEPARTS UNIT
(From DD Form 689)
SCREENER LOCATION
TIME PATIENT ARRIVES |
TIME ENCOUNTER BEGINS |
TIME PATIENT LEAVES |
|
|
|
SCREENER LOCATION
CHIEF COMPLAINT
DURATION
PATIENT RESIDENCE |
|
|
VITAL SIGNS |
|
|
|
|
|
|
|
||
( ) BARRACKS |
( ) POST HOUSING |
TEMPERATURE |
|
|
|
|
ALLERGIES |
|
||||
( ) OFF POST |
( |
) TRANSIENT |
PULSE |
|
BP |
|
RESP |
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
FIRST VISIT FOR THIS COMPLAINT ( |
) YES ( ) NO IF NO, WAS RETURN SCHEDULED/REQUESTED BY CARE PROVIDER? |
|||||||||||
( ) YES ( ) NO |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
ALGORITHM/CODE |
|
|
|
ALGORITHM/CODE |
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
ALGORITHM SUMMARY |
|
|
ALGORITHM SUMMARY |
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
COMMENTS (Reasons for referral, method of referral, hospital appointments,
PATIENT'S IDENTIFICATION (Use mechanical imprint if available, for typed or written entries give: Name, SSN, Unit, Sex, Birthdate and
Duty Phone)
FINAL DISPOSITION |
|
|
||
( ) |
I - PHYSICIAN STAT |
( ) |
IV - SELF CARE PROTOCOL |
|
( |
) |
II - PA STAT |
( |
) V - HOSP CLINIC REFERRAL |
|
( |
) III - PA |
|
|
AIDMAN'S SIGNATURE & CODE
AUDITOR'S INITIALS & DATE
DA FORM |
PREVIOUS EDITIONS OF THIS FORM ARE OBSOLETE. |
USAPPC V1.00 |
TAB |
TAB TAB |
TAB |
TAB |
TAB |
RECORD OF ACUTE MEDICAL CARE
(Entries on this record should be restricted to further evaluation and treatment of complaint(s) screened)
DATE
2ND CARE LOCATION
TIME PATIENT ARRIVES
TIME ENCOUNTER BEGINS
TIME PATIENT LEAVES
SIGNATURE OF HEATH CARE PROVIDER
SIGNATURE OF MEDICAL SUPERVISOR
AUDITOR'S INITIALS AND DATE
SPECIAL INSTRUCTIONS
This form will be utilized in lieu of SF 600 (Health
REVERSE OF DA FORM |
USAPPC V1.00 |